Just enough time for me to draw attention to some important happenings about to take place in the world of mental health nursing. Tomorrow evening (June 12th) Alan Simpson delivers this year’s Skellern Lecture and Malcolm Rae receives his Journal of Psychiatric and Mental Health Nursing Lifetime Achievement Award. Here are the flyers for these linked events, both taking place at City University London:
Catching my eye earlier this week was an interview in The Guardian with Jane Cummings, Chief Nursing Officer (CNO) with a place on NHS England‘s National Commissioning Board. Under the header, ‘Nobody can say care is brilliant all the time’ the article opened with this understated quote:
‘It was very clear that nursing was getting a bit of a bad name and it felt like the profession was being quite beleaguered and criticised.’
Nursing certainly has been under siege. Responses to descriptions of poor care have included the three year Compassion in Practice strategy introduced by the CNO and her Director of Nursing counterpart at the Department of Health, Viv Bennett. It is in this document that the 6Cs are described:
The proposals for HCA experience prior to joining a pre-registration nursing programme are underpinned by a set of assumptions about nursing education and selection of prospective students that is deeply flawed. It paints a picture of students who have never had experience of caring and little interest in patient care, picked out for their grades by a group of academics in total isolation from staff working in clinical services. The message from current practices and the NMC Standards that govern them is that this mental picture needs to change. In particular, the assumption that students are not recruited for their values and that students do not have prior care experience are incorrect.
What about the nub of the proposal: that exposure to the clinical frontline as a HCA will create better nurses? The evidence here is equivocal at best. What care experience does seem to do is give prospective students exposure to the reality of working in healthcare and so it may reduce attrition from programmes. But there is also evidence that working as a HCA can socialise prospective students into poor practice and inhibit their development as nurses. Unless the evidence is looked at carefully, these proposals could therefore embed rather than challenge poor patient care. As the pilots of the proposals are developed, care must be taken both to recognise existing practice and carefully test assumptions against the evidence.
So, nursing practice and nursing education are in the spotlight, and the profession has responded. Senior members have asserted a set of fundamental values (the 6Cs), and in resisting the year-as-an-HCA idea have reminded people of the differences between what nurses and other health care workers do.
We are therefore in good company. Other workers know what it is like to be told they have collectively fallen short, and understand how it feels to have their status undermined. Status-knocking sometimes happens because professional groups engage in ongoing division of labour skirmishes, as I have drawn attention to on this site before. But nursing’s current predicament, in which we are charged with having a ‘compassion deficit’ and sacrificing a commitment to care in the pursuit of academic credentials, is different.
Perhaps nurses have finally lost enough of the untouchable, ‘angel’, image (no bad thing, in my view) to now be viewed as ‘just’ another professional group in whom trust is conditional. We control entry to our profession, expect degrees from new entrants, have university departments and lead interprofessional teams and whole services within the NHS. In turn, we must expect to face questions when things go wrong, and to justify why we do practice and education in the ways that we do. For the record, I strongly favour system explanations for what happens in the health service (including its failures), see no evidence that student nurses no longer care and much prefer practitioners to be educated than not. But I also think we must expect, and should prepare for, more ‘bashing’ in the future.
Not much time for adding to the blog at the mo’, but enough to note that it was good to have spent this morning with the MHRNC Service User and Carer Partnership Research Development Group. This is an important initiative, and today’s meeting brought together user representatives, charity sector staff, colleagues from Involving People and academics. I’m something of a late arrival to the group, and lots of interesting work has already been done: including a research priority-setting exercise. More to follow in due course, I’m sure.
Here’s what will probably be a final Hay Festival-related post. Last Thursday the Nobel Laureate Professor Sir John Sulston chaired a discussion titled The Next Big Thing. This began with four researchers talking about what they do: Alison Rust, a volcanologist; Zita Martins, an astrobiologist; Nicole Grobert, a nanotechnologist; and Jenny Nelson, a physicist working on materials for solar cells.
All gave fascinating talks, and exemplified the art of conveying complex ideas to the interested but non-specialist listener. And who doesn’t want to hear about supervolcanoes (for the record, they’re bad news, and are definitely best avoided)? Or amino acids from space, the practical applications of graphene or comparing different ways of capturing energy from the sun?
This discussion has since got me thinking about the Next Big Things in nursing and midwifery research (and mental health nursing research in particular). Generally nurses do not do fundamental or basic science, and are not in the business of discovering how bits of the natural world work. So, no volcanoes or extraterrestrial chemicals for us. But practical applications of health-related technologies, and exploring and comparing different ways of doing health work? That’s more up our street, I think, even if graphene and solar power are unlikely to immediately feature.
River Wye, Builth Wells
To the applications-of-technology and exploring-and-comparing questions which might be asked within mental health nursing I would personally add some others related to the examination of health and health care experiences. We know that mental health nurses do ‘people work’ in a big way, spend much of their time coordinating (or ‘articulating’) complex trajectories of care and are often present during service users’ critical junctures. There are applications of skill and technology in this, and how nurses do their work and the effects this has are wide-open areas for study. COCAPP, as I’ve mentioned on this site before, is aiming to distil the components of care planning and care coordination associated with recovery-oriented and personalised mental health services, and is a great example of applied research in this broad field. I’d like to think that its findings will, in some way, be directly useful to practitioners and others in the fullness of time.
Thinking of Graham Thornicroft’s recent editorial on the poor physical health of people using mental health services, referred to on this blog here, if asked to give their research priorities now perhaps some would make a case for researchers and practitioners to combine their efforts to seriously improve this situation. I know there are people working in this area already, but given the magnitude of the problem it seems to deserve some serious new investment. And how about extending research into the mental health nursing contribution to the vital care of older and vulnerable people, including those with dementia? Again, there are people, such as John Keady, doing this already, but possibly not in sufficient numbers. Or research in the area of quality improvement and safety? And what about workforce research, including studies into factors sustaining nurses’ resilience to provide care in conditions of adversity?
However they might be identified and emerge I suspect that any Next Big Thing candidates for nursing research will be the products of sustained collaborations. To return to last Thursday’s four discussants at Hay: all were explicit about interdisciplinarity, and the importance of crossing boundaries to do high quality research aimed at answering ‘big questions’. There are established academic mental health nurses doing this already (I’m thinking of people like Len Bowers, Karina Lovell, Patrick Callaghan and Alan Simpson), but more of us need to make friends with colleagues possessing specific substantive and methodological expertise relevant to our intended studies. Depending on the questions at hand this might mean finding collaborators with disciplinary backgrounds in various of the social and physical sciences and in the humanities, and if necessary with experience in the practical conduct of clinical trials, qualitative investigation and so on. Crucially, and arguably most importantly, it also means forging meaningful collaborations with people with experience of using services, whose priorities are the ones which really matter.
Further to my last post referring to Raymond Tallis’ staunch defence of the NHS, a second excellent health service-related talk at Hay was Andrew Edgar’s. Andrew is a philosopher at Cardiff University, and on Tuesday he gave a customarily considered account of (amongst other things) the principles underpinning the NHS and how these contrast with those associated with health care systems elsewhere in the world. I particularly appreciated Andrew’s view of the NHS as being more than a way of simply (simply?) funding and delivering health care. It is a unifying force, embodying the majority view that some things are best paid for and organised collectively. Insurance based systems, as Andrew observed, are abhorrent to many in the UK because they treat health care as a commodity and pay insufficient regard to need.
Beyond the principles, as Andrew also pointed out, lie some difficult day-to-day health service realities. These include the existence of rationing (which clearly exists, but is rarely talked about in an open way), and the fact that the system retains a capacity to grind down, and sometimes even brutalise, those who work within it. But opening the service up to market forces, along the lines happening in England with the passing of the Health and Social Care Act 2012, is no remedy. Note my reference to ‘England’ here. Quite correctly, in my view, Andrew was careful to talk of not one but four ‘NHSs’ reflecting the divergence in systems across the different countries.
Yesterday at the Hay Festival I heard Raymond Tallis deliver a strong attack on the coalition government’s ‘redisorganisation’ of the NHS in England. The Health and Social Care Act 2012 has opened the NHS to the market in unprecedented fashion. Tallis talked of the dominance of private providers on clinical commissioning groups, and gave examples of patients being cherrypicked by organisations more concerned with profit than with meeting need. He also contrasted the upheaval with pre-2010 general election promises by both the Conservatives and the LibDems not to unleash major top-down change on the health service.
Tallis was critical of his own profession (medicine) for having failed to coordinate opposition to the legislation as it worked its way through parliament. He did, though, pick out and praise Clare Gerada of the RCGP for leading the resistance. I’m aware that the RCN was against the proposed Act, but I’m not sure that nurses as a group were particularly visible during the debates.
The first question from the audience asked what needs to be done to prevent the Act infecting Wales. The balance of politics here is different than in England, but it was a good question nonetheless.
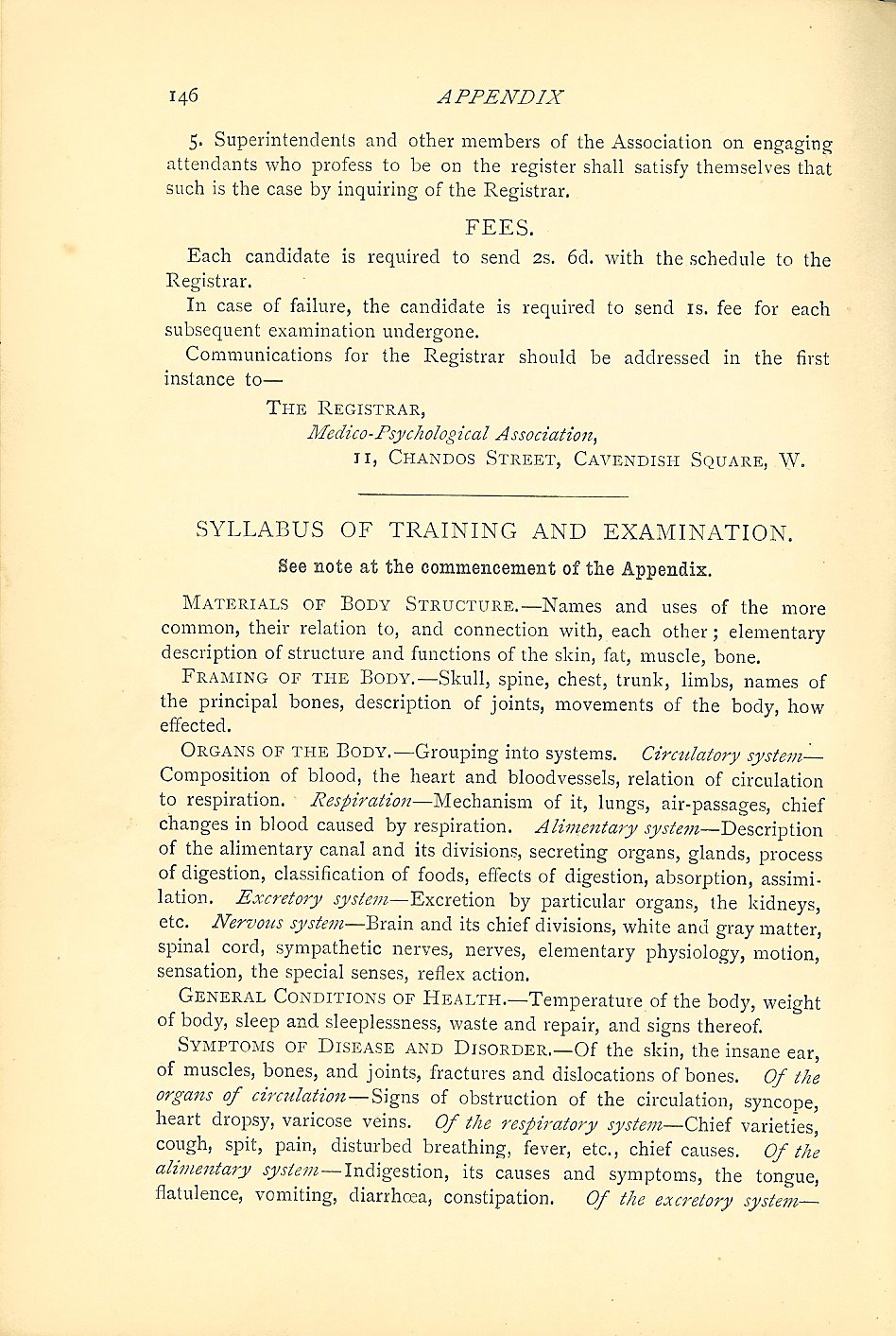
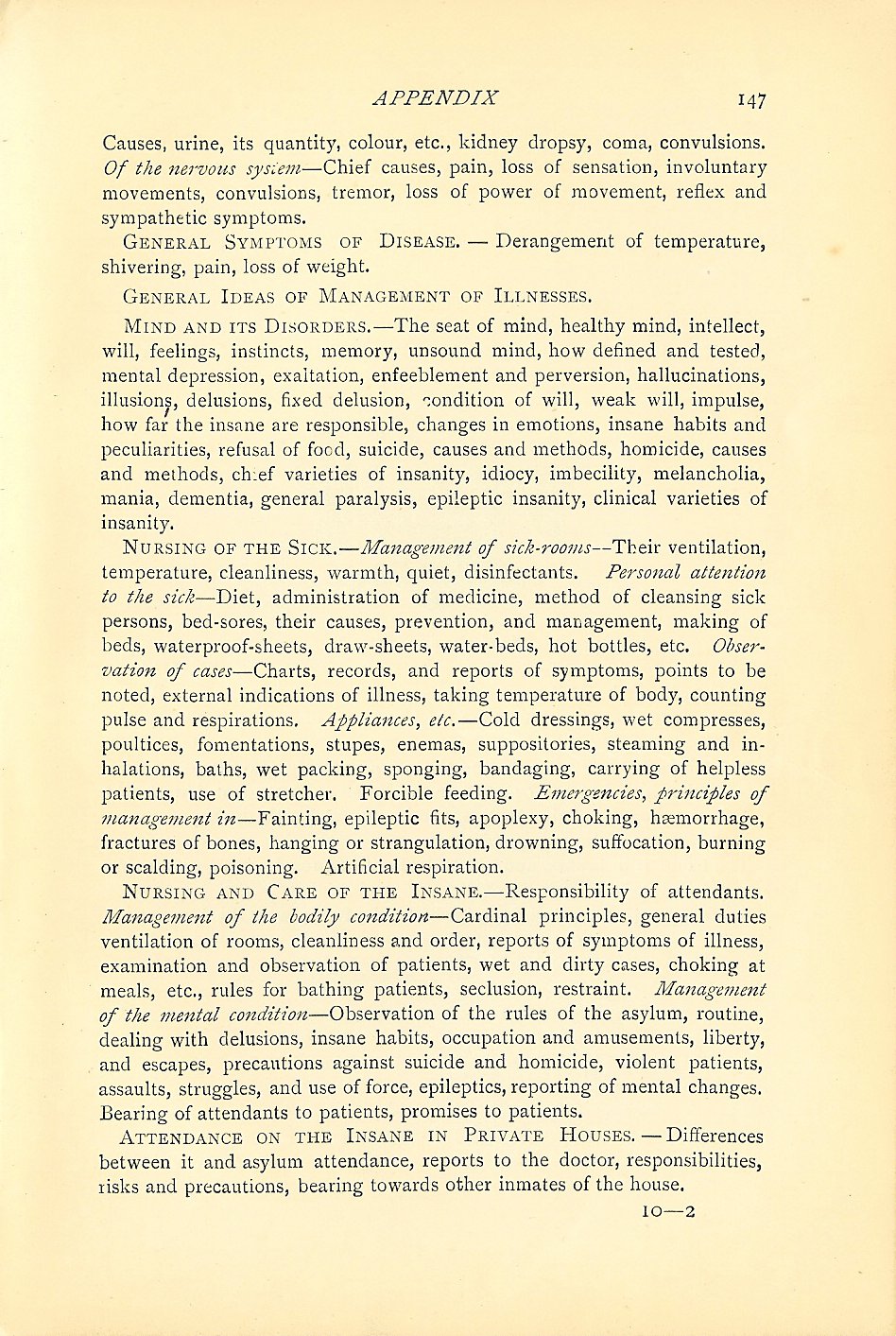
For students up and down the country it is examination season. Whilst students of mental health nursing are busy submitting their dissertations, writing up their reflective essays and achieving their practice-based ‘competencies’ I thought it might be interesting to share the ‘Regulations for the Training and Examination of Candidates for the Certificate of Proficiency in Nursing and Attending on the Insane’. I have scanned these from my copy of the Red Handbook:
In uploading these pages I have just noticed the mention (on page 147, the last-but-one reproduced above) of ‘Attendance of the insane in private houses’. Is it stretching things too far to suggest this as an early reference to community mental health nursing?
I also notice how much these regulations refer to the assessment and maintenance of bodily health (although I have no idea whatsoever what might be meant by ‘the insane ear’, a phrase appearing on page 146). Earlier this week, writing in an editorial for the BMJ Graham Thornicroft described the excess mortality of people with mental health problems as ‘a human rights disgrace’. He’s right, and whilst I’m glad we’re out of the age of the asylum and of ‘attending on the insane’ we might yet learn something from an historic nursing syllabus which placed emphasis on the importance of physical well-being.
Time this morning for a brief post drawing attention to two excellent opportunities for people with personal experience of using mental health services to contribute to COCAPP.
Information about the positions can be found by clicking this link, then following the link onwards to ‘Managerial, Administration and Support’. The opportunities are listed as vacancy number 1007BR, ‘Service User Project Assistants’.
A brief post with no bearing on work matters whatsoever. Yesterday evening, in the two hours before sunset (which was just after 9pm), a perfect opportunity was presented to take in the simple pleasures of walking the Taff Trail. This is one of the places I also like to run, though for the last few weeks I’ve been nursing a sore Achilles and have, therefore, been resisting.
This part of the world is criss-crossed with disused railway lines, harking back to South Wales’ industrial heritage. Check out the photo here, which was taken yesterday on the flat, mile-long, stretch leading from the Penrhos Cutting to the bottom of the steep hill which climbs above Castell Coch.
This second photo was taken on the same stretch looking towards Craig yr Allt, which remains one of my most favourite places of all.
A brief, early morning, rant. I’m all for open access, but this morning – and most certainly not for the first time – I received an unsolicited and entirely unwanted email inviting me to submit a paper to an open access journal. The editor asked me to write in an area I know nothing about, and informed me that if my manuscript is accepted for publication I shall have to pay an author processing charge (APC). I did the only thing possible in the circumstances, which was to delete the email.
I don’t mind a bit of academic spam, but I despair at the poor targeting and am a little affronted at the invitation being so baldly attached to a fee. I still don’t get why APCs are (often, but admittedly not always) as high as they are. Had I bitten at this morning’s ‘opportunity’, having done all the hard graft I would have needed to part with around £950 (so my online currency converter tells me). Where’s that going, then? Not to the peer reviewers, who like authors are not paid directly for their efforts.


 It is also in this general context, but specifically following the publication of the
It is also in this general context, but specifically following the publication of the 





 A brief post with no bearing on work matters whatsoever. Yesterday evening, in the two hours before sunset (which was just after 9pm), a perfect opportunity was presented to take in the simple pleasures of walking the
A brief post with no bearing on work matters whatsoever. Yesterday evening, in the two hours before sunset (which was just after 9pm), a perfect opportunity was presented to take in the simple pleasures of walking the  was taken on the same stretch looking towards
was taken on the same stretch looking towards 