This month brought, for me, the welcome return of face-to-face conferences. First, I was pleased to have received an invitation earlier in the year to deliver a keynote lecture at the RCN International Nursing Research Conference 2022, which took place at the Royal Welsh College of Music and Drama on September 5th and 6th. Rather than speak about any one, particular, study I used this as an opportunity to travel over a larger programme of research in the mental health field, pulling out underpinning ideas and key messages along the way.
Boiled down, my talk revolved around four ideas: health care can be thought of as a complex system; complex health systems can be understood through the study of cases, existing at different ‘levels’ of organisation (macro, meso and micro); to appreciate cases of health care system complexity it makes sense to use a plurality of analytic and methodological approaches; and research of this type demands a collaborative, stakeholder-informed, approach. These will be familiar themes to readers of this blog site. My talk at the RCN event, however, represented the most sustained effort I’ve made to date to articulate the principles and practices underpinning the research programme I have been involved in, to synthesise the main lessons learned, and to pull out some overarching observations. At some point it would make sense to write all of this up in an article.
Hot on the heels of the RCN International Nursing Research Conference came the 28th International Mental Health Nursing Research Conference, which took place at St Catherine’s College, Oxford, on September 8th and 9th. St Catherine’s was the home for the Network for Psychiatric Nursing Research Conference, as this event was originally known, for many years: returning there earlier this month seemed fitting after the two online editions of the event which happened in 2020 and 2021. I was pleased to be part of a symposium presenting findings from three NIHR-funded studies into mental health crisis services. Led By Dr Nichola Clibbens, this included a talk by Nicola and Michael Ashman drawing from their (and their colleagues’) realist synthesis of how, for whom and in what circumstances different community mental health crisis services work. Also featuring was a presentation from Professor Steve Gillard and Dr Katie Anderson on mental health decision units in acute care pathways. Third in the linked series of presentations was my talk summarising findings from an evidence synthesis, led by Dr Nicola Evans, into crisis responses for children and young people aged 5 to 25.
More generally, I very much appreciated the opportunity at both these events to renew my connections with friends and colleagues, and to meet and hear new people with interesting things to say. In the case of MHNR2022, particular thanks are due to the organising committee, which brought this conference together under the umbrella of Mental Health Nurse Academics UK without a dedicated events team in support.
Currently I’m serving a term as Director of Postgraduate Research in the School of Healthcare Sciences, which means I have responsibilities for our PhD and our Doctorate in Advanced Healthcare Practice (DAHP) programmes. For aspirant researchers a doctoral degree is a necessary qualification, with the PhD culminating in the production of a thesis of some 80,000 words whilst the DAHP in Cardiff combines taught modules and a shorter thesis of no more than 50,000 words. In the School we have numbers of students in the thesis stage of their DAHP degrees, but this particular programme no longer recruits new entrants. The PhD, though, continues to attract people from the UK and around the world and information on it can be found here.
October is the first opportunity in each academic year for postgraduate student enrolment, and compared to the numbers of people commencing their undergraduate and taught postgraduate studies our newly starting students are small in number. This is to be expected, but this also takes me to the general observation that the health professions need many more people to get involved in research and knowledge creation.
Information on developing research careers in the mental health field can be found at the NIHR Incubator for Mental Health Research website. There is lots of value here, including advice on first steps, on sources of funding, and on finding support and mentorship. There are case studies, too, of people from a range of backgrounds and at different stages of their research careers (including people studying for doctorates), and a whole section aimed at nurses.
Meanwhile, the Royal College of Nursing has launched the Annie Altschul Collection, an online repository of doctoral degrees completed by mental health nurses. The repository is searchable, and is also themed, with hyperlinks to the full text of each included thesis where these are available.
I take the view that ‘everything is connected to everything else’, to use a phrase I recently learn is attributed to Leonardo da Vinci. More on him later.
Over the past week I’ve been involved in industrial action as part of #UCUStrikesBack. What I’m not going to do in this post is to explain why university staff are currently on strike, largely because this has already been adequately covered elsewhere (for example, see here and here). Instead, I want to share some picket-line reflections linking what happens in universities with what happens in the health service. These are connections which are not being made frequently enough, including by some who should know better.
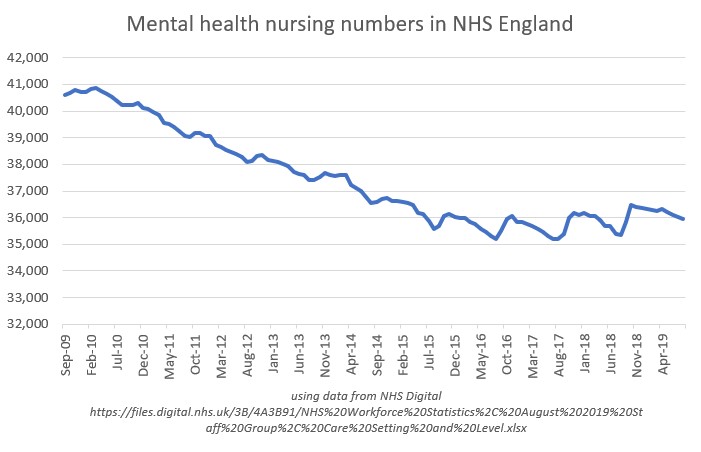
As a mental health nurse academic I am acutely aware of the perilous position occupied by my profession in the NHS, with reports from earlier in 2019 pointing to a loss of 6,000 mental health nurses in NHS England since 2009. Below is a graph, created using NHS Digital data, which starkly reveals the current situation:
As an aside, data of this type are not published here in Wales. They should be. In any event, quite correctly much concern has been expressed about this startling decline in the workforce, with mental health nursing now singled out as a group needing particular help to improve both recruitment and retention.
Reflecting my position as a health professional academic I hold joint membership of the University and College Union (UCU) and the Royal College of Nursing (RCN). The RCN, along with other health service unions like Unite and Unison, is trying to reverse the crisis facing the nursing workforce. It is campaigning on safe staffing, has published a manifesto to assist nurses wanting to interrogate prospective parliamentary candidates ahead of the December 2019 general election, and through its Fund our Future campaign is lobbying government to reverse the removal of tuition fee and living cost support for students of nursing in England.
These campaigns are important. So far, however, in its public pronouncements the RCN has failed to make the necessary connections between working conditions in universities and the present and future education of student nurses. Put simply, an adequate supply of educated, evidence-minded, person-centred nurses demands an adequate supply of secure, well-supported, fairly paid nurse educators and researchers. Nurse academics typically have career trajectories which are significantly different from those in other fields, with implications for their recruitment, retention and development. The modern norm for historians, physicists and sociologists seems to involve years of precarious, post-doctoral, employment characterised by repeated short-term contracts before landing (if ever) much sought-after full-time academic posts. In contrast, with some exceptions nurses are generally recruited into higher education by dint of their practitioner expertise, their posts linked to the servicing of courses of professional study. This was certainly how it was for me: my academic career commenced with an initial series of short-term employment contracts associated with the leading of a post-qualification course for community mental health nurses. In all universities, nurse academics can soon find themselves carrying major teaching and course management responsibilities, often for programmes and modules of study which run more than once across a single year. Demanding education and education-related workloads can squeeze out time for research, scholarship and wider engagement, in workplaces which traditionally value productivity in these areas for the purposes of career progression.
Expanding the number of nurses to fill the gaps which now exist, for which the RCN and others are rightly campaigning, requires thought and careful planning. In the run-up to the general election both are in short supply as nursing numbers become reduced to political soundbites. More student nurses must mean more nurse academics, but in any future rounds of staff recruitment potential entrants will have their eyes wide open. The erosion of university pensions relative to pensions in the NHS does nothing to encourage those contemplating the leap from health care into higher education (or, at least, into that part of the sector in which the Universities Superannuation Scheme predominates). Very reasonably, those considering future careers as nurse academics will also want to weigh up the appeal of doing work which is undoubtedly creative and rewarding with what they will hear about workloads, developmental opportunities and work/life balance.
I also learn, this week, that Leonardo da Vinci saw the making of connections as necessary in order that we might see the world as it truly is. In my working world, education, research and practice are intimately intertwined. It is disappointing that these connections are being missed by organisations which campaign on the state of nursing and the NHS, but which do not (as a minimum) also openly acknowledge the concerns that nursing and other academics have regarding the state of universities. Right now, some words of solidarity and support would not go amiss.
Belated happy new year. Visiting the Royal College of Nursing headquarters in London last Friday ahead of a meeting of the Network for Psychiatric Nursing Research (NPNR) conference committee (more on that below) gave me an opportunity to pop into the ‘Out of the Asylum’ exhibition. I’m glad I did. Texts, photographs and other artefacts illustrate the history of mental health nursing.
Here are some of the pictures I took. These include a photo of the RCN’s copy of a sixth edition of the Red Handbook, displayed alongside nurses’ badges, a Bethlem Royal Hospital pamphlet, a syringe and other items of interest. For more on the Red Handbook see this earlier post, along with this post which includes material from my copy of a fourth edition of the same. Another picture relates a set of regulations for the bathing of patients.
One of the display boards makes the observation that ‘few mental health nurses now wear uniforms’. As an unfortunate aside, this may need some future updating. From what I’m hearing, the historic trend towards mental health nurses wearing everyday clothes at work is reversing, with numbers of NHS trusts and health boards contemplating a return to uniforms. I regret that. But sticking with the exhibition…
…a final photograph I’m reproducing here is the front sheet of an early 1930s examination paper. Look hard and you’ll see questions on bones, asphyxia and antiseptics (amongst other things).
The NPNR planning meeting, this being the purpose of my trip, was a productive one. This year’s event (the 22nd) will be taking place in Nottingham on September 15th and 16th. I’ll add more on this when I can, and include some regular updates on this site.
In other news, I find myself engaged in a prolonged period of doctoral student activity. I’ve examined a number of theses in and out of Cardiff in recent months, and have sat with students during their vivas as either supervisor or independent chair. This term has been particularly packed. Plenty of writing has also been taking place: papers and reports are being written from COCAPP, RiSC and Plan4Recovery, and from completed theses I have helped to supervise. Data generation in COCAPP-A has almost concluded, and new research ideas are taking shape. Exciting times, if a little frenetic.
November 17th was the School of Healthcare Sciences’ annual postgraduate research student symposium. This was, as usual, an excellent showcase for the PhDs and Professional Doctorates ongoing in the School. Follow this link for information on individual students and their projects.
I’ll write more about this in a separate post, but on Thursday November 19th, in Cardiff City Hall I was pleased to receive the Research in Nursing Award for 2015 at the Royal College of Nursing in Wales Nurse of the Year event. I appreciated very much the kind messages from esteemed friends and colleagues received via Twitter, text and email. I am particularly happy to have won this award as a mental health nurse, again being reminded of the need for investment in both mental health services and in research to find out what helps.
The 21st Network for Psychiatric Nursing Research (NPNR) conference took place on Thursday and Friday, September 17th and 18th 2015, with the theme of ‘Building new relationships in mental health nursing: opportunities and challenges’. The occasion was a fine one, with just short of 200 people in attendance. For those not able to make it but wanting to know more, the programme can still be found here and the book of abstracts here.
I’ve been on the NPNR scientific and organising committee this year, courtesy of my membership of Mental Health Nurse Academics UK. This afforded me the chance to welcome delegates at the conference opening, and to draw attention to the just-breaking news of Professor Len Bowers’ planned retirement at the start of 2016. Len has been an inspirational mental health nurse researcher: more on this later.
#NPNRselfie with Karina Lovell
Introduced by Professor Liz Hughes as day one conference chair, this year’s keynotes commenced with Professor Karina Lovell giving an overview of the current state of knowledge in remote psychological therapies. Karina is a world leader in research into interventions for people with commoner mental health problems such as depression and anxiety, as well as being actively involved in services and practice through her work with organisations like Anxiety UK and others. For an example of important new research in this area check out the REEACT trial into computerised CBT for people with depression. This is an important study which Karina both referenced in her talk, and is actively involved in.
Dr Geraldine Strathdee, NHS England’s National Clinical Director for Mental Health, delivered a second keynote on using mental health intelligence. She praised the work of nurses, and made a strong case for mental illness prevention. Geraldine also reminded delegates of the high rates of premature mortality of people living with mental health difficulties, and the continued exclusion of many from employment. As routes to improvement she pointed to leadership, and the value of data to benchmark and drive up standards.
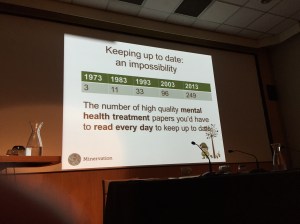
Keeping up with the evidence: an impossibility?
Day one’s final keynote presentation was delivered by André Tomlin, founder of the Mental Elf website and author of this pre-conference blogpost. André is an information scientist, who illustrated the challenge of keeping up-to-date with the evidence using this slide. Podcasts, social media, tweetchats and other new technologies are all part of André’s solution to the challenge of information overload, and as strategies to help plug the leaky evidence pipeline. The National Elf Service, of which the Mental Elf is a part, plays a big part in this area; for an overview of what’s on offer, here’s one of André’s videos:
Therapeutic approach, or therapeutic alliance?
Chair for day two was Professor Doug MacInnes, one of whose duties was to introduce Professor Shôn Lewis from the Institute of Brain, Behaviour and Mental Health at the University of Manchester as the deliverer of the conference’s fourth keynote lecture. Shôn spoke about current approaches to the care and treatment of people with psychosis and schizophrenia, using findings from the non-commercial CATIE and CUtLASS trials to suggest that newer antipsychotics are generally no better than first generation antipsychotics. Shôn also referenced the SoCRATES trial to evidence the idea that outcomes are associated with the quality of the therapeutic alliance, rather than with the specific therapeutic approach used. SoCRATES, I have now discovered, compared the effectiveness of (1) CBT plus routine care, (2) supportive counselling plus routine care and (3) routine care alone for people with schizophrenia. Shôn devoted the last part of his presentation to ClinTouch (a mobile phone app to record and upload symptoms) and CareLoop (which is testing if ClinTouch can be connecteded to NHS IT systems and to everyday practice).
Mark Brown about to begin his talk
#NPNR2015’s final keynote was delivered by Mark Brown, and the full text of his talk can be read here. Mark edited One in Four magazine, and is now development director of Social Spider, runs the Day in the Life project and is part of the team behind the WeMHNurses Twitter meeting place. Drawing on personal experience of its usefulness he described digital technology as less of a possible future than an unfolding present. One example of tech in action, which Mark referred to in his talk, is his own Doc Ready website. This was designed to help people prepare for discussions with doctors about their mental health difficulties.
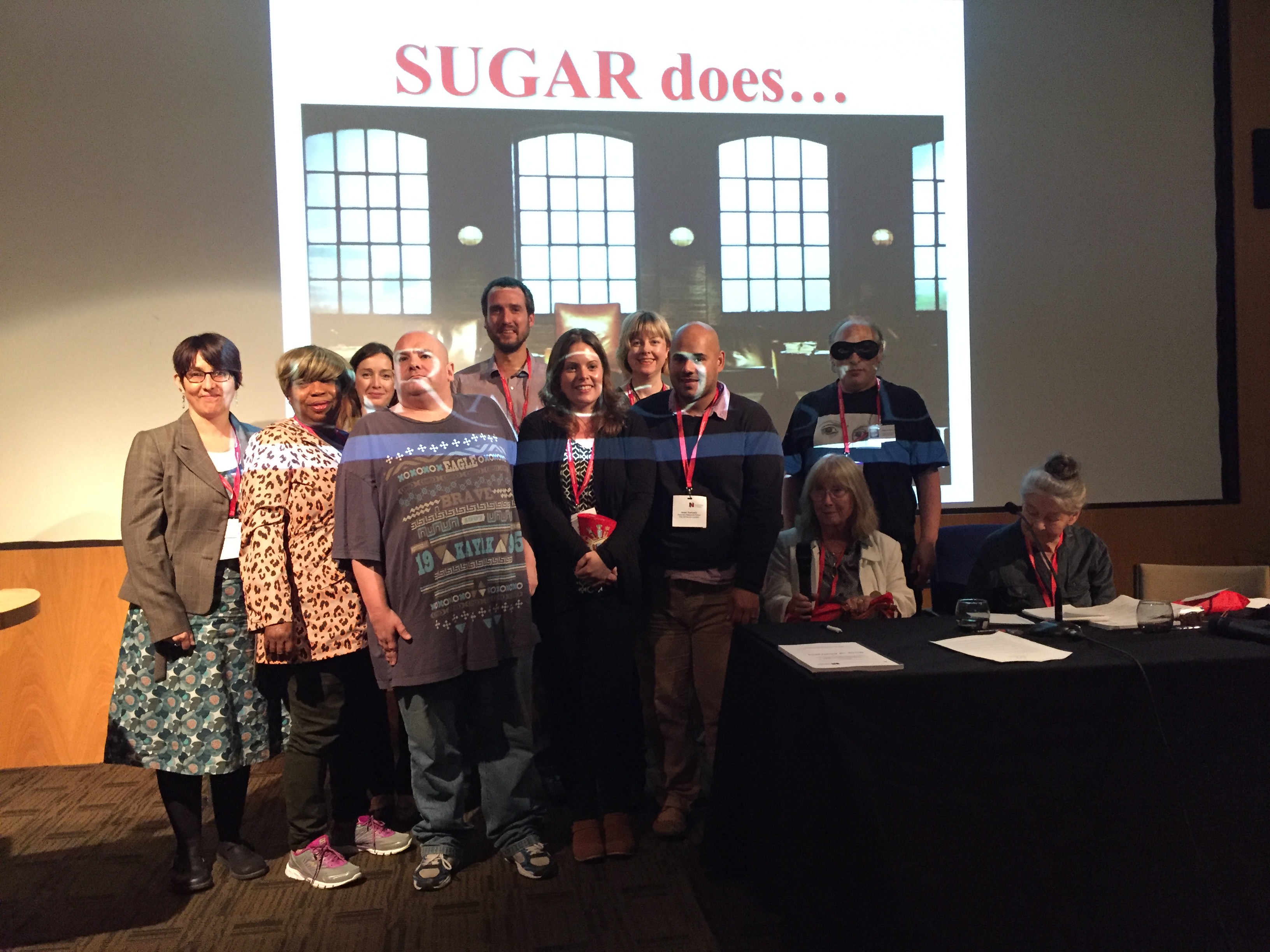
SUGAR does Dragons’ Den
That’s summary enough of the keynotes. From the concurrent sessions I participated in, chaired or observed I’ll first start with the SUGAR meets Dragons’ Den workshop. Three volunteers – Jason Hickey, Laoise Renwick and Cher Hallett – pitched their research ideas to SUGAR members. In the event, SUGAR offered their time and support to all three, but also voted Cher’s plans (on intramuscular injections) as the best of the batch. In the second concurrent I’m picking out, Julian Hunt, Alan Meudell and Michael Coffey presented reflections from Plan4Recovery. This project, which I’m also part of, is examining shared decision-making and social networks for people using secondary mental health services. And, finally, a word about our COCAPP symposium. This started with an overview paper from Alan Simpson, was followed by a presentation from Michael Coffey titled, ‘Ordinary risks and accepted fictions: how contrasting and competing priorities work in risk assessment care planning’ and concluded with a paper from Sally Barlow and me on participants’ views and experiences of recovery and personalisation.
The RCN’s history of mental health nursing exhibition
Organised by Laoise Renwick, this year for the first time the NPNR conference featured a poster trail. This worked well. Displayed posters were themed, and during lunchtime on day two guided delegates took opportunities to speak with those associated with them. Along the way I spotted some interesting posters from the RCN, drawing attention to an upcoming history of mental health nursing exhibition (organised with lots of help from Ian Hulatt) about to launch in London.
Finally, a word on Len Bowers. At Doug MacInnes’ invitation, Len took to the lectern during the afternoon of day two to confirm his upcoming retirement and his plans for the future. These include (we learned) playing the flute, travel, photography and electronic music-making. Very nice. Len is a generous, principled and humble man whose contribution to creating new knowledge for mental health nursing has been immense. Take Safewards as an example. This is Len’s NIHR-funded programme grant, findings from which are changing practice in the UK and around the world. That’s some achievement, in my book. We wish him well.
Working with the charity Rethink Mental Illness, and drawing on publicly available data, the RCN shows how (since 2010) the number of staffed mental health hospital beds across all four countries of the UK has reduced. The number of nurses working in NHS mental health services has also fallen, those remaining being revealed as an ageing group. Year on year, an increasing proportion is shown to be over the age of 50.
Here’s a chart showing reductions in the mental health nursing workforce, which I’ve extracted from page 16 of the report:
And, right at the front of the document, I see a clear case for investment contained in these recommendations which I reproduce word-for-word:
1) Governments must ensure there is equal
access to mental health services and that
the right treatment is available for people
when they need it.
2) Governments and NHS providers must
ensure that the commitment to parity of
esteem is directly reflected in the funding,
commissioning of services, workforce
planning, and patient outcomes.
3) Local commissioners and health boards
must make available enough local beds
to meet demand.
4) The principle of least restriction must
be embedded across all mental health
services. Detention under mental health
legislation should always be based on
clinical opinion and never be a result
of local failures to provide appropriate
care. Due to the significant increase in
detentions under the Mental Health Act
there should be a national objective set
to reduce detention rates in England.
5) There must be a consistent shift across
the UK from inpatient acute care to
community-based services which
recognises that prevention and early
intervention results in better outcomes,
reduces the pressure on acute services,
and reduces the overall cost to the NHS
in the long term.
6) Urgent action must be taken to address
the workforce shortages. Resources must
be committed to training and recruiting
enough mental health nurses who are able
to deliver specialist care in the changing
health and social care landscape.
7) NHS providers must invest in the current
mental health nursing workforce.
Band 6, 7 and 8 mental health nurses
should be developed to become advance
practitioners to deliver effective
recovery-led care in mental health
services.
8) There must be a sustainable and
long-term workforce planning strategy
which acknowledges the current
challenges facing the mental health
nursing workforce.
Early news of this year’s International Network for Psychiatric Nursing Research conference, and a call for abstracts, have just appeared. The event takes place at Warwick University on September 18th and 19th, and more information can be found by following this link. With support once again from both the Royal College of Nursing and Mental Health Nurse Academics UK this promises to be a special occasion, this being the 20th running of this esteemed event.



 As an aside, data of this type are not published here in Wales. They should be. In any event, quite correctly much concern has been expressed about this startling decline in the workforce, with mental health nursing now singled out as
As an aside, data of this type are not published here in Wales. They should be. In any event, quite correctly much concern has been expressed about this startling decline in the workforce, with mental health nursing now singled out as 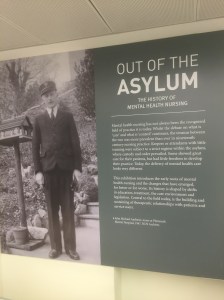 Belated happy new year. Visiting the Royal College of Nursing headquarters in London last Friday ahead of a meeting of the Network for Psychiatric Nursing Research (NPNR) conference committee (more on that below) gave me an opportunity to pop into the ‘Out of the Asylum’ exhibition. I’m glad I did. Texts, photographs and other artefacts illustrate the history of mental health nursing.
Belated happy new year. Visiting the Royal College of Nursing headquarters in London last Friday ahead of a meeting of the Network for Psychiatric Nursing Research (NPNR) conference committee (more on that below) gave me an opportunity to pop into the ‘Out of the Asylum’ exhibition. I’m glad I did. Texts, photographs and other artefacts illustrate the history of mental health nursing. Here are some of the pictures I took. These include a photo of the RCN’s copy of a sixth edition of the Red Handbook, displayed alongside nurses’ badges, a Bethlem Royal Hospital pamphlet, a syringe and other items of interest. For more on the Red Handbook see this
Here are some of the pictures I took. These include a photo of the RCN’s copy of a sixth edition of the Red Handbook, displayed alongside nurses’ badges, a Bethlem Royal Hospital pamphlet, a syringe and other items of interest. For more on the Red Handbook see this 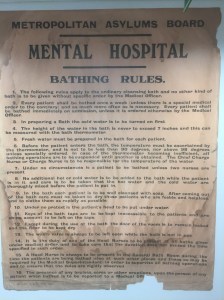
 The NPNR planning meeting, this being the purpose of my trip, was a productive one.
The NPNR planning meeting, this being the purpose of my trip, was a productive one.  Lots of interesting things to relate in this post. November 13th saw
Lots of interesting things to relate in this post. November 13th saw  I’ll write more about this in a separate post, but on Thursday November 19th, in
I’ll write more about this in a separate post, but on Thursday November 19th, in 




 Here’s a post to draw attention to the
Here’s a post to draw attention to the 
 Early news of this year’s International Network for Psychiatric Nursing Research conference, and a call for abstracts, have just appeared. The event takes place at Warwick University on September 18th and 19th, and more information can be found by following
Early news of this year’s International Network for Psychiatric Nursing Research conference, and a call for abstracts, have just appeared. The event takes place at Warwick University on September 18th and 19th, and more information can be found by following 