Here’s a link to my first post for a new Cardiff University Mental Health Blog. The content will be broadly familar to people who have dipped into my personal blog in the past, insofar as I have chosen to say something general about doing mental health services research.
Working in collaboration with colleagues across the UK, including with people who have directly used services, researchers in the School of Healthcare Sciences at Cardiff University study mental health systems.
Clicking the hyperlink above, which appears beneath the brief snippet of text, will take you to the full piece. There are already some interesting other posts on the site, too, including a piece by Mike Owen written as an opener.
Background: In the UK, concerns about safety and fragmented community mental health care led to the development of the care programme approach in England and care and treatment planning in Wales. These systems require service users to have a care coordinator, written care plan and regular reviews of their care. Processes are required to be collaborative, recovery-focused and personalised but have rarely been researched. We aimed to obtain the views and experiences of stakeholders involved in community mental health care and identify factors that facilitate or act as barriers to personalised, collaborative, recovery-focused care.
Methods: We conducted a cross-national comparative study employing a concurrent transformative mixed-methods approach with embedded case studies across six service provider sites in England and Wales. The study included a survey of views on recovery, empowerment and therapeutic relationships in service users (n = 448) and recovery in care coordinators (n = 201); embedded case studies involving interviews with service providers, service users and carers (n = 117) and a review of care plans (n = 33). Quantitative and qualitative data were analysed within and across sites using inferential statistics, correlations and framework method.
Results: Significant differences were found across sites for scores on therapeutic relationships. Variation within sites and participant groups was reported in experiences of care planning and understandings of recovery and personalisation. Care plans were described as administratively burdensome and were rarely consulted. Carers reported varying levels of involvement. Risk assessments were central to clinical concerns but were rarely discussed with service users. Service users valued therapeutic relationships with care coordinators and others, and saw these as central to recovery.
Conclusions: Administrative elements of care coordination reduce opportunities for recovery-focused and personalised work. There were few common understandings of recovery which may limit shared goals. Conversations on risk appeared to be neglected and assessments kept from service users. A reluctance to engage in dialogue about risk management may work against opportunities for positive risk-taking as part of recovery-focused work. Research to investigate innovative approaches to maximise staff contact time with service users and carers, shared decision-making in risk assessments, and training designed to enable personalised, recovery focused care coordination is indicated.
People may be interested to learn that COCAPP will also be the subject of a Mental Elf blog and podcast in a week or so’s time:
And, for those wanting the fine-grained detail, there is always our main report to the National Institute for Health Research (NIHR) Health Services and Delivery Research (HS&DR) Programme.
Time, just about, to use a bus journey across Cardiff en route to the University Hospital of Wales site (for the purposes of teaching) to post an update on recent activities.
There’s lots to say. Projects I’ve blogged about on this site (COCAPP, COCAPP-A, Plan4Recovery) are now being written up. Our main findings paper from COCAPP appears imminently in BMC Psychiatry. Alan Simpson, as lead author, completed checking the proofs of this in the last few days so we know it’s on its way. Michael Coffey has lead authored a COCAPP paper addressing risk; earlier this week this was accepted for publication in Health Expectations. Further papers will follow, as they will in the future from COCAPP-A. I’ll make a point of posting about each as they appear. Plan4Recovery has been about shared decision-making and social approaches to care, and here, too, work on a first publication is well underway.
Meanwhile, Therapeutic skills for mental health nurses edited by Nicola Evans and me has just been published by Open University Press. This is a fine text indeed (though I say so myself), which we hope proves particular useful to students.
A big highlight of the last few weeks has been the award of a doctorate to my colleague and (now former) student Pauline Tang. Pauline used qualitative methods to investigate the use of electronic patient records in a medical assessment unit, and you can read her thesis here. And talking of doctorates: Mohammad Marie, writing with Aled Jones and me, has a second paper from his study of resilience in Palestinian community mental health nurses about to appear: this one in the International Journal of Mental Health Nursing.
Right! I’m off the bus and walking to a classroom. Time to fly, and to remind myself that it is perhaps better to post more frequently than to cram so much into a single, short, piece like this.
Clicking the image of the front page of Jane Davies‘ PhD in this post will download the complete text of this newly completed doctorate. Danny Kelly and I were Jane’s supervisors, and for a flavour of her study and its findings here is its abstract:
This thesis is the result of an in-depth study, which explored the experience of choice and control in decision making when five young people developed and were subsequently treated for cancer. The study was underpinned by the sociological theories of agency and structure against the backdrop of the developmental nature of adolescence and emerging adulthood. The experience of the disease was situated at a time when these young people were in the process of developing their early adult life plans and were at a fundamental crossroad in the life cycle. The diagnosis and subsequent treatment for cancer at this juncture impacted significantly on the lives of these five young people and those close to them.
Exploratory case studies were utilised in an attempt to examine more specifically each young person’s choice, intentionality, control and freedom in deciding all aspects of decision making, beginning with the onset of symptoms followed by diagnosis and treatment. Interviews, observations and documentary analysis were instigated to generate data. Multiple sources were selected to generate further insights and these included family, partners, friends and health care professionals who were close to the young people during their experience.
Three overarching themes were identified during analysis of the data: ‘life then’, ‘life interrupted’ and ‘life reclaimed’. Key elements of these themes included a number of complex and interrelating factors which were interwoven within the everyday lives of the young people. In the ‘life then’ phase, ‘holding on’ to agency prior to diagnosis and the importance of close and intimate relationships was illuminated. In ‘life interrupted’, agentic power during treatment, in terms of the range of decision making and the complexity of the parental role, were prominent. In ‘life reclaimed’ the ‘different but determined’ nature of young people’s behaviour and re-aligned agency was transparent as they made their way towards the end of treatment.
The findings culminated in the illumination of individual trajectories relating to the fluctuating nature of agency during the cancer experience. These incorporated the three overarching themes as three sequential phases. Commonalities in this regard were also identified across the five cases. Several discussions with practice colleagues resulted in the formulation of potential ways in which ultimately these trajectories might be applied to practice in the future.
For those who may need additional persuading: further to my post last week on qualitative research, Jane’s thesis is another example of why this type of study needs to be done. This is an excellent doctorate. The data therein were carefully and sensitively generated, analysed and written up. Jane has already lead authored this paper, which appeared in the Journal of Advanced Nursing last year. Expect more to follow.
Technological failure meant I was unable to participate in this week’s Mental Elf campfire discussion, What has qualitative research ever done for us? The context for the event was the recent decision by the BMJ to reject a paper submitted for publication by members of the McGill Qualitative Research Group on the grounds that qualitative research reports are of low priority. This, the BMJ editors added, is because they are downloaded and cited less often than are reports of quantitative research. The BMJ communication conveying this news to the McGill team was posted on social media, triggering significant protest and then a letter to the BMJ making the case for qualitative methods and urging an editorial rethink.
These kinds of debates over the relative value of different research approaches flare up from time-to-time. Sixteen years ago Philip Burnard and I wrote a paper on the emergence of two camps within mental health nursing. We characterised these with reference to a quantitative/qualitative divide, and made a case for rapprochement and synthesis.
In the event, this week’s campfire which I missed was a sensible and informed one, with excellent speakers. The recording can be viewed here:
For the record, the exemplar piece of qualitative mental health research which I had prepared to talk about is Strauss and colleagues’ Psychiatric ideologies and institutions. I wrote a short piece about this book in 2014, on the occasion of its fiftieth birthday. My view remains that many of the observations made within it are as relevant now as they were in 1964. Ideas and practices, for example, remain contested.
This week’s Mental Elf campfire discussion also included some commentary on the use of mixed methods. COCAPP and COCAPP-A demonstrate the value of combining quantitative and qualitative approaches, and reveal how data from surveys, interviews, observations and documentary review can be fruitfully brought together. This type of study is becoming increasingly popular, informed by the idea that different research questions (of a type which might be brought together in a single project) simply require different methods to answer them. This is a position I remain comfortable with.
And so we press on. I’ve been involved in lots of writing lately, as projects yield papers. As per my usual practice, as these appear in journals I’ll aim to write posts on this blog about them and include links to open access versions as I am able. Thanks for reading, and feel free to comment.
Happy April. Here’s a new venture for me: blogging for the Mental Elf, part of the National Elf Service. This is a fine site indeed, which André Tomlin set up in 2011 with the aim of helping people find ‘just what you need to keep up-to-date with all of the important and reliable mental health research and guidance’.
Here’s a summary of my first post, which can be read in full by following the link at the bottom.
Ben Hannigan writes his debut blog on the CADET cluster RCT, which investigates the clinical effectiveness and cost-effectiveness of collaborative care for depression in UK primary care.
The article is titled Mental health needs and services in the West Bank, Palestine and has this for an abstract:
Background: Palestine is a low income country with scarce resources, which is seeking independence. This paper discusses the high levels of mental health need found amongst Palestinian people, and examines services, education and research in this area with particular attention paid to the West Bank.
Methods: CINAHL, PubMed, and Science Direct were used to search for materials.
Results and conclusion: Evidence from this review is that there is a necessity to increase the availability and quality of mental health care. Mental health policy and services in Palestine need development in order to better meet the needs of service users and professionals. It is essential to raise awareness of mental health and increase the integration of mental health services with other areas of health care. Civilians need their basic human needs met, including having freedom of movement and seeing an end to the occupation. There is a need to enhance the resilience and
capacity of community mental health teams. There is a need to increase resources and offer more support, up-to-date training and supervision to mental health teams.
Further papers from Mohammad’s study will follow, and I’ll aim to post updates as work progresses.
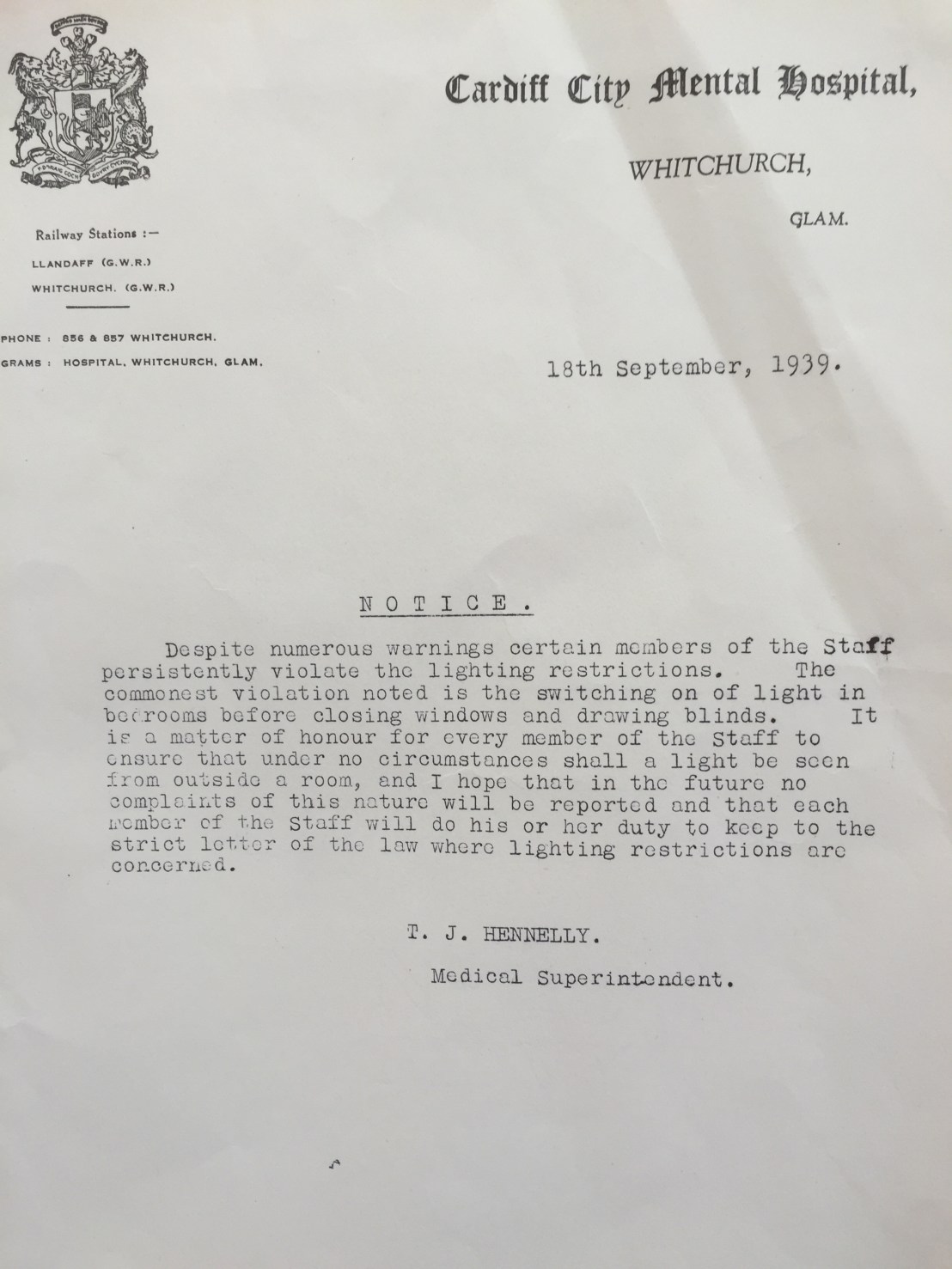
Last Friday afternoon I took the opportunity to visit the End of an Era exhibition at Whitchurch Hospital. The hospital opened in 1908, for more than a century providing inpatient mental health care for the people of Cardiff and its surroundings. Now, all clinical staff and current inpatients are about to move to a newly built facility in the grounds of Llandough Hospital in the Vale of Glamorgan.
The exhibition was the work of the Whitchurch Hospital Historical Society, and was excellent. Extracts from the written archives, images and objects were on display, painting a fascinating picture of life inside the hospital over the decades. I hope a permanent home is found for at least some of this in the future. Here, for now, are some of the photographs I took.
Meanwhile, here is what people have been saying about the new Hafan y Coed unit which is about to open at the start of April 2016:
In this post I’ll largely confine myself to some thoughts on the mental health workforce and on the place of nurses within this. Yesterday’s discussions in this area exercised MHNAUK members greatly. Proposed changes to the occupational mix to be found within mental health services, debates over nursing numbers and safe staffing, and new arrangments for the funding of education have the potential to trigger significant turbulence in an already-complex system of care. MHNAUK members rightly identified how the appearance of a new associate nurse role, sitting in between health care support workers and registered nurses, will trigger unrest. This is always the case when professional jurisdictions come under pressure (see here and here for papers I have co-written which expand on this point). In this current case, some registered nurses will see new associates as a threat to their hard-won jurisdiction. At a time when nurses are pressing for safe staffing, some are likely to argue that the introduction of associates will also open the door to role substitution and eventual reductions in numbers of registered nurses, thereby threatening both quality and safety.
Should associate nurses appear, we can be certain that plenty of inter-occupational jostling will take place as support workers, associates and registered nurses (amongst others) negotiate their relative positions and assert control over areas of work. In this regard, abstract descriptions of the tasks which new associates will (and will not) be permitted to carry out will provide only the most limited of guides. Differentiations between who does what will inevitably be hammered out in the workplace.
And what of the cross-UK implications for all of this, given that the Department of Health’s associate nurse announcement is for England only? To me it is unclear how new associates will be regulated, or how transferable their future qualifications might be should any wish to move to, say, Wales. Across the four countries of the UK important differences are appearing in the ways people are prepared for health care practice, and in the funding of this. Student nurses will pay fees in England from next year, but student nurses in Scotland will not and will continue to receive a bursary. Here in Wales (unless I’ve been asleep and have missed a piece of essential news), we will need to wait until after our forthcoming Assembly elections and the formation of a new Welsh Government for an announcement on future financial arrangments for nursing education. Perhaps we’ll hear more about the shape of the future Welsh NHS workforce then, too.
Over on the #NPNR2016 website the call for abstracts has now been published. The conference takes place on September 15th and 16th, at the Nottingham Conference Centre, and our theme for this year’s event is mental health across the life course. Here’s some more information:
The NPNR conference is the leading mental health nursing conference in the UK. This year our 22nd conference will explore the challenges faced by mental health nurses in delivering evidenced-based compassionate care across the life course. We will consider both the complexity of issues faced by individuals throughout the life course, and also how well services and nurses meet the mental health needs of the people they collaborate with .
Once again, our intention is to provide an event where you can engage and critically debate issues (from education, practice and research) of relevance to the way care is provided and received. The NPNR conference is the place for mental health nurses and those we work with to present and learn new knowledge, therefore we encourage you to submit your research and practice development initiatives.
The conference also provides a great opportunity to participate in discussion so that you leave the conference informed, enlightened and with new energy to engage with the challenges ahead. Alongside our expert speakers, great practice development and research papers the conference promotes a friendly and welcoming atmosphere that has been the hallmark of NPNR for over 20 years.




 Last Friday afternoon I took the opportunity to visit the
Last Friday afternoon I took the opportunity to visit the 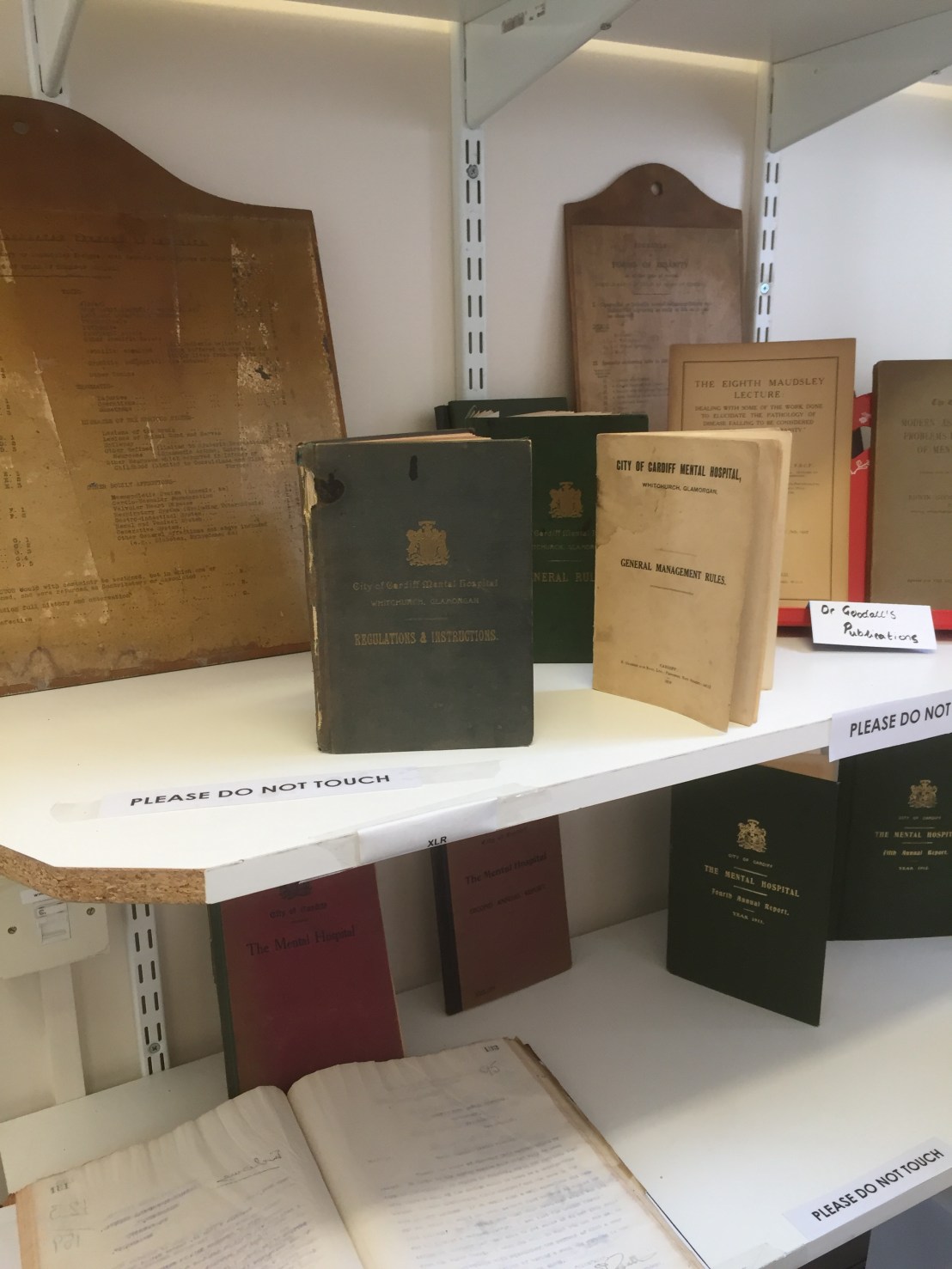


 Over on the
Over on the 