This new paper you need to read. You also can, because it is published in gold open access form and is therefore free to download to anyone with an internet connection. Lead authored by Michael Coffey, and arising from the larger COCAPP study (see also here, here and here), it draws on qualitative data to examine in detail what staff, service users and carers say about risk assessment and management. Here’s the abstract:
This new paper you need to read. You also can, because it is published in gold open access form and is therefore free to download to anyone with an internet connection. Lead authored by Michael Coffey, and arising from the larger COCAPP study (see also here, here and here), it draws on qualitative data to examine in detail what staff, service users and carers say about risk assessment and management. Here’s the abstract:
Background
Communication and information sharing are considered crucial to recovery-focused mental health services. Effective mental health care planning and coordination includes assessment and management of risk and safety.
Objective
Using data from our cross-national mixed-method study of care planning and coordination, we examined what patients, family members and workers say about risk assessment and management and explored the contents of care plans.
Design
Thematic analysis of qualitative research interviews (n = 117) with patients, family members and workers, across four English and two Welsh National Health Service sites. Care plans were reviewed (n = 33) using a structured template.
Findings
Participants have contrasting priorities in relation to risk. Patients see benefit in discussions about risk, but cast the process as a worker priority that may lead to loss of liberty. Relationships with workers are key to family members and patients; however, worker claims of involving people in the care planning process do not extend to risk assessment and management procedures for fear of causing upset. Workers locate risk as coming from the person rather than social or environmental factors, are risk averse and appear to prioritize the procedural aspects of assessment.
Conclusions
Despite limitations, risk assessment is treated as legitimate work by professionals. Risk assessment practice operates as a type of fiction in which poor predictive ability and fear of consequences are accepted in the interests of normative certainty by all parties. As a consequence, risk adverse options are encouraged by workers and patients steered away from opportunities for ordinary risks thereby hindering the mobilization of their strengths and abilities.
Reported here is one of the most important sets of findings arising from the COCAPP study. Diana Rose has written a post on the article, which is scheduled to appear on the inestimable Mental Elf site next week. I’m very much looking forward to reading that.
Follow @benhannigan



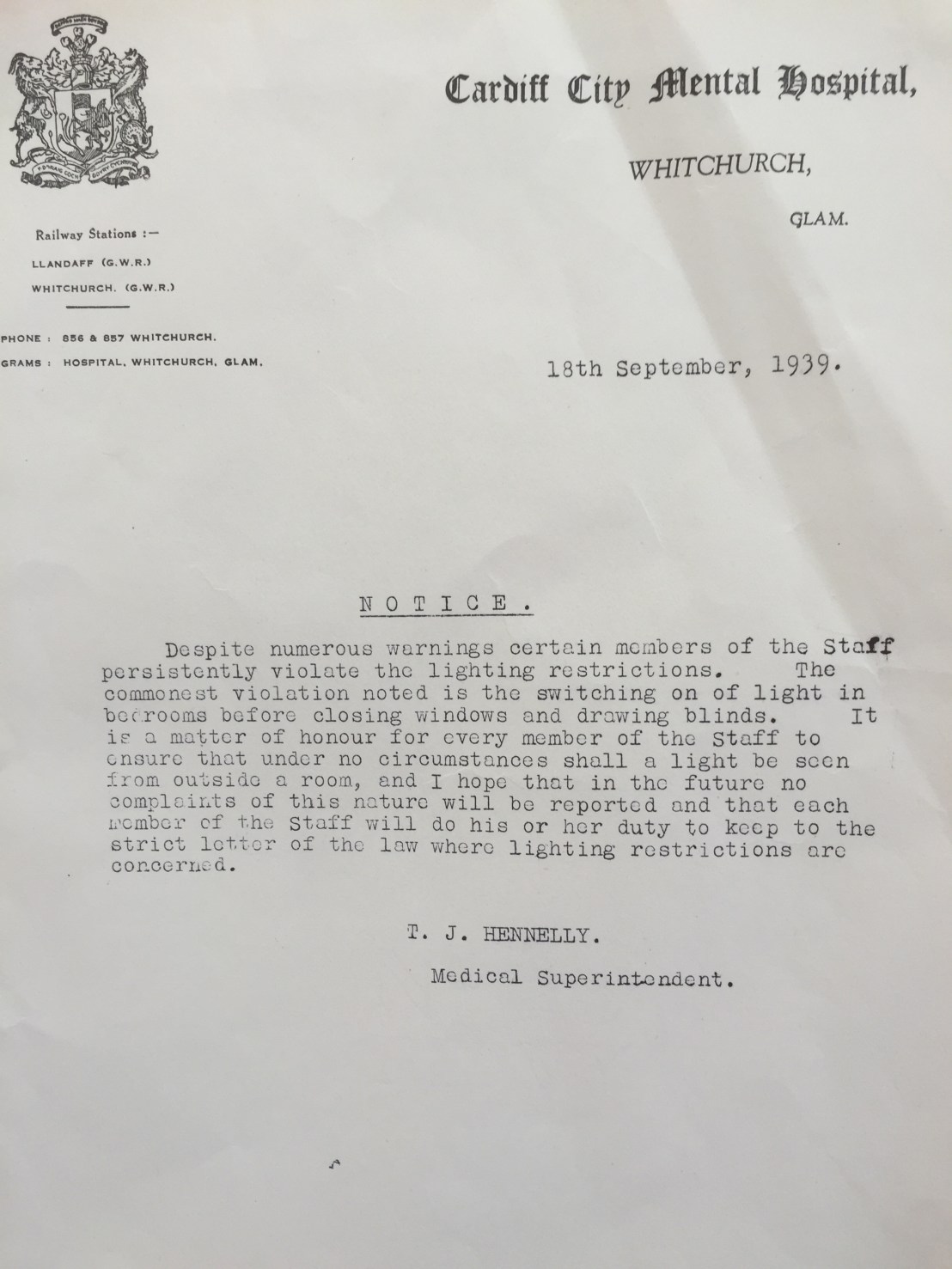
 Last Friday afternoon I took the opportunity to visit the
Last Friday afternoon I took the opportunity to visit the