Most of today I spent in the School of Healthcare Sciences’ Bringing us back together postgraduate research symposium, and very much enjoyed hearing about the projects which doctoral students in the School are engaged in. The event was opened by Eluned Morgan, Minister for Health and Social Services in the Welsh Government, who spoke in support of the health care workforce and of the importance of research which makes a difference to the care and treatment which people receive.
The talks which followed demonstrated, faultlessly, how applied the School’s postgraduate research projects are. Amongst our 90 or so research students are people investigating the improvement of clinical interventions. Many are also examining the experiences of people with long-term conditions and the support they receive, whilst others are exploring aspects of the workforce and the organisation and delivery of services.
This symposium, set up by Dr Tina Gambling who served with great distinction as the School’s Director of Postgraduate Research prior to her untimely passing in November 2020, is (or has been) an annual event, the organisation of which is always led by students with support from staff. The organising committee for today did a very fine job, as did the session chairs and speakers. The Bringing us back together theme, too, felt right.
The REF moves in long cycles. The first took place in 2014, replacing the Research Assessment Exercise which had previously run every five or so years from the middle of the 1980s to 2008. For the 2021 Research Excellence Framework (REF2021) universities made submissions to up to 34 units of assessment, each covering a subject area and each operating underneath one of four main panels. Most research conducted by nursing academics in the REF2021 census period will have been submitted to the Allied Health Professions, Dentistry, Nursing and Pharmacy unit of assessment (UOA). In each UOA, expert panels reviewed the quality of three separate components within each submitting university’s return: outputs, impact and environment. An output might be a single journal article, or perhaps a book or monograph, assessed by members of the relevant expert panel for its ‘originality, significance and rigour’. The assessment of impact involved the expert review of university-submitted case studies exemplifying the ‘reach and significance’ of research beyond academia. Environment involved review of how far each university was enabling the ‘vitality and sustainability’ of excellent research in the subject area.
Suffice to say, the REF is a big deal for universities, subject areas and researchers, with very considerable resources being devoted by institutions to secure as favourable a set of outcomes as possible. As a process it has both its supporters and its detractors, with a summary of controversies surrounding the REF appearing on this Wikpedia page. Debates aside, results from REF2021 have now been published, with the data searchable both by university and by unit of assessment. Main panel reports have also appeared, with more data (including the detail of each submission to each UOA) expected in due course. Both the Times Higher and the Wonkhe teams have produced independent analyses of what the results mean, with the Council of Deans of Health publishing a response highlighting how ‘research undertaken by our members [as submitted to the Allied Health Professions, Dentistry, Nursing and Pharmacy UOA] tackles real life health challenges facing patients, health services and local communities as well as addressing wider societal challenges and global health inequalities.’
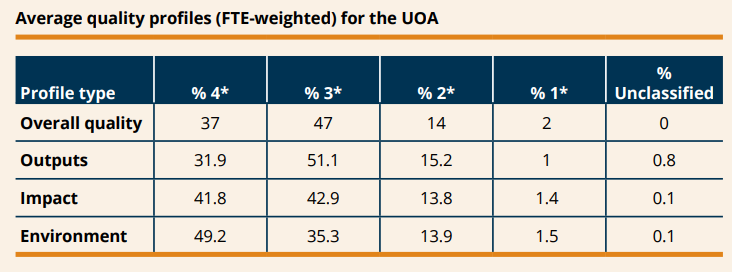
Extracted directly from the Overview report by Main Panel A and Sub-panels 1 to 6, here is a summary of the average assessed quality profile of research submitted to the Allied Health Professions, Dentistry, Nursing and Pharmacy UOA:
Here, 4* refers to ‘world-leading’, 3* to ‘internationally excellent’, 2* to ‘internationally recognised’ and 1* to ‘nationally recognised’. Overall, then, this table gives lots to celebrate, pointing to allied health, nursing and related research being done to a very high quality, and making a significant difference beyond academia. This much is acknowledged explicitly in the UOA-specific overview report, but so too is a note on the importance of continued investment in research capacity-building and in supporting early careers. I find it hard to disagree with that sentiment. Whilst REF outcomes come round only once every six or seven years, the work of enabling and growing research capability is a constant.
With funding from the National Institute for Health Research comes the opportunity (and indeed, the requirement) to produce a detailed monograph reporting on all aspects of the project which has been supported. The Health and Social Care Delivery Research monograph arising from the MENLOC evidence synthesis, about which I have added various posts on this site, has now appeared. As with all NIHR project reports, this is free to download.
Here is the plain English summary:
In this study we brought together evidence from research, policies, guidance and case studies in the area of end-of-life care for people with severe mental illness. End-of-life care refers to the help given to people with life-threatening conditions in their expected last 12 months of life. Severe mental illness refers to a range of issues for which care is usually provided by specialist mental health services.
An advisory group, which included people who had experience of mental health and end-of-life care, helped us throughout our project. We searched research databases, journals and online sources. We assessed research articles for their quality and summarised their content. In one review we combined content from research with content from policy and guidance. In another review we combined the content of the case studies. We wrote synthesis statements summarising the research evidence, and assessed how much confidence decision-makers should have in these statements.
We included 104 documents overall. We synthesised research, policy and guidance under themes reflecting their content: the structure of mental health and end-of-life care services; professional practice; providing and receiving care; and living with severe mental illness. We synthesised case studies under themes relating to delays in diagnosis, making decisions, treatment futility, supporting people and the experience of care.
Our project has implications for care. The evidence suggests that partnerships should be built between mental health and end-of-life care staff, and that people should be supported to die where they choose. Care staff need education, support and supervision. A team approach is needed, including support for advocacy. Physical health care for people with severe mental illness needs to be improved so that life-threatening conditions can be recognised sooner.
Future research should involve people with severe mental illness at the end of life and their carers. Research is also needed to evaluate new ways of providing and organising care.
Here is our second published paper from the MENLOC project, which has synthesised what is known about end of life care for people with severe mental health problems. This article, led by Michael Coffey, reports on our theming of the evidence derived from previously-published case studies. The paper is in BMJ Open, is open access, and has this as its abstract:
Objectives: People with severe mental illness (SMI) have significant comorbidities and reduced life expectancy. The objective of the review reported in this paper was to synthesise material from case studies relating to the organisation, provision and receipt of care for people with SMI who have an end-of-life (EoL) diagnosis. Design: Systematic review and thematic synthesis. Data sources: MEDLINE, PsycINFO, EMBASE, HMIC, AMED, CINAHL, CENTRAL, ASSIA, DARE and Web of Science from inception to December 2019. Supplementary searching for additional material including grey literature along with 62 organisational websites. Results: Of the 11 904 citations retrieved, 42 papers reporting 51 case studies were identified and are reported here. Twenty-five of the forty-two case study papers met seven, or more quality criteria, with eight meeting half or less. Attributes of case study subjects included that just over half were men, had a mean age of 55 years, psychotic illnesses dominated and the EoL condition was in most cases a cancer. Analysis generated themes as follows: diagnostic delay and overshadowing, decision capacity and dilemmas, medical futility, individuals and their networks, care provision. Conclusions: In the absence of high-quality intervention studies, this evidence synthesis indicates that cross-disciplinary care is supported within the context of established therapeutic relationships. Attention to potential delay and diagnostic overshadowing is required in care provision. The values and preferences of individuals with severe mental illness experiencing an end-of-life condition should be recognised.
A not-uncommon research strategy in health and social care research is to generate different types of data and, through some process of transformation, bring these together into a coherent whole. The idea here is that combining data produces a more complete, detailed, analysis than can be created using one type of data alone. For example, in my doctorate, which focused on the system of mental health care and the division of labour, I conducted lots of qualitative interviews but also used written records as a source of data and observed people going about their day-to-day work. What people say, what people do, and what people write about they’ve done are not the same thing: knitting together a rich, or ‘thick’, description of a social setting is helped when different classes of data are available to be drawn upon. In more recent studies of care planning and coordination (see here and here) the research teams I’ve been a part of have variously combined interviews, documentary review, questionnaires and observations.
In a slow-burn kind of way, over a period of many months I’ve been working with members of the 3MDR project team to bring together data of very different types. The 3MDR study, led by Jon Bisson, is something I’ve written about before and involved examining the efficacy of a novel intervention for people with post-traumatic stress disorder. Across the project overall three, distinct, classes of data were generated: outcomes, derived from clinician-assessed and self-reported standardised measures; psychophysiological, including breathing and heart rate, walking pace, words and phrases used by participants during therapy, plus subjective unit of distress scores; and qualitative, namely post-therapy interviews where people talked about their views and experiences. Working particularly closely, in the first instance, with Robert van Deursen and Kali Barawi our task has been a mixed-methods data synthesis to explore the interrelationships between people, interventions and context and to investigate how factors within these three domains interact in specific outcome typologies.
This has been an interesting and challenging project, and we’re not yet done. Whilst many of the ideas underpinning this analysis are familiar ones (complexity, interconnections, the search for patterns) the combined dataset we’re mixing together is an unusual one. This work is also proving to be a reminder of how much can be found out through the detailed study of relatively small numbers of participants. Our data relate to ten people only, but our total dataset is both comprehensive and varied. At some point (but not quite yet) we’ll have a paper ready for journal submission, and I’ll be able to share more on this site.
In recent months I’ve been part of a team, led by Nicola Evans, bringing together the evidence in the area of responses for children and young people in mental health crisis. Our working definition of a ‘crisis response’ has been the provision of a service in response to extreme psychosocial distress, which for children and young people may be provided in any location such as an emergency department, primary care, a specialist or non-specialist community service, a school, a college, a university, a youth group, or via a crisis support line. Our objectives have been:
To critically appraise, synthesise and present the best available evidence on the organisation of crisis services for children and young people aged 5 to 25 years, across education, health, social care and the third sector.
To determine the effectiveness of current models of mental health crisis support for children and young people.
To explore the experiences and perceptions of young people, families and staff with regards to mental health crisis support for children and young people aged 5 to 25 years.
To determine the goals of crisis intervention
As a project team we’ve been informed by a stakeholder advisory group, and have cast a wide net by searching not only for research but also other relevant evidence including guidance, case studies and more. Methodologically, therefore, this review bears comparison with others I’ve previously written about on this site including the RiSC study and MENLOC. More on this crisis care evidence synthesis to follow in due course.
Currently I’m serving a term as Director of Postgraduate Research in the School of Healthcare Sciences, which means I have responsibilities for our PhD and our Doctorate in Advanced Healthcare Practice (DAHP) programmes. For aspirant researchers a doctoral degree is a necessary qualification, with the PhD culminating in the production of a thesis of some 80,000 words whilst the DAHP in Cardiff combines taught modules and a shorter thesis of no more than 50,000 words. In the School we have numbers of students in the thesis stage of their DAHP degrees, but this particular programme no longer recruits new entrants. The PhD, though, continues to attract people from the UK and around the world and information on it can be found here.
October is the first opportunity in each academic year for postgraduate student enrolment, and compared to the numbers of people commencing their undergraduate and taught postgraduate studies our newly starting students are small in number. This is to be expected, but this also takes me to the general observation that the health professions need many more people to get involved in research and knowledge creation.
Information on developing research careers in the mental health field can be found at the NIHR Incubator for Mental Health Research website. There is lots of value here, including advice on first steps, on sources of funding, and on finding support and mentorship. There are case studies, too, of people from a range of backgrounds and at different stages of their research careers (including people studying for doctorates), and a whole section aimed at nurses.
Meanwhile, the Royal College of Nursing has launched the Annie Altschul Collection, an online repository of doctoral degrees completed by mental health nurses. The repository is searchable, and is also themed, with hyperlinks to the full text of each included thesis where these are available.
Here is a first publication from the MENLOC study, reporting on a synthesis of research, policy and guidance in the area of end of life care for people with severe mental illness. This is in the journal Palliative Medicine, and the abstract is here:
Background: Parity of esteem means that end-of-life care for people with severe mental illness should be of equal quality to that experienced by all. Aim: To synthesise international, English language, research and UK policy and guidance relating to the organisation, provision, and receipt of end-of-life care for people with severe mental illness. Design: A mixed methods systematic review was conducted following the Evidence for Policy and Practice Information and Coordinating Centre approach and informed by a stakeholder group. We employed thematic synthesis to bring together data from both qualitative and quantitative studies, and from non-research material. We assessed the strength of synthesised findings using the Confidence in the Evidence from Reviews of Qualitative Research (CERQual) and Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approaches. Data sources: Ten electronic databases were searched from inception to December 2019, along with 62 organisational websites. Quality appraisal was conducted using Critical Appraisal Skills Programme checklists or other study design-specific alternatives as necessary. Results: Of the 11,904 citations retrieved, 34 research publications were included plus 28 non-research items. The majority of research was of high or acceptable quality. An overarching synthesis including 52 summary statements, with assessments of confidence in the underpinning evidence, was produced using four themes: Structure of the system; Professional issues; Contexts of care; and Living with severe mental illness. Conclusions: Implications for services and practice reflect evidence in which there is a high degree of confidence. Partnership should be developed across the mental health and end-of-life systems, and ways found to support people to die where they choose. Staff caring for people with severe mental illness at the end-of-life need education, support and supervision. End-of-life care for people with severe mental illness requires a team approach, including advocacy. Proactive physical health care for people with severe mental illness is needed to tackle problems of delayed diagnosis.
Continuing from this recent post celebrating the publishing of papers from doctorates I’ve had a hand in supervising, here now are links to Nicola Savory’s PhD and to a first article from this in the journal Midwifery. Nicola is a midwife, and in her thesis (funded by RCBC Wales) used quantitative and qualitative methods to investigate women’s mental health needs in the antenatal period.
Nicola’s whole-thesis summary is this:
Background: Existing research on poor perinatal mental health largely focuses on recognition and treatment of postnatal depression. Consequently, there is a need to explore antenatal mental health. Aim: To assess poor mental health prevalence in pregnancy, its relationship to sociodemographic characteristics, self-efficacy and perceived support networks. To understand experiences and barriers preventing women with mental health problems from receiving help and explore midwives’ understanding of their role. Method: Questionnaires were completed by women in early pregnancy. A subset identified to have mental health problems, were interviewed in late pregnancy to explore their experiences and barriers to receiving care. Midwives completed questionnaires exploring their experiences of supporting women with mental health problems and focus groups further discussed the issues raised. Results: Amongst participants (n=302), the Edinburgh Postnatal Depression Scale (EPDS) identified 8.6%, and the Generalised Anxiety Disorder Assessment (GAD-7) 8.3%, with symptoms of depression or anxiety respectively. Low self-efficacy (p=0.01) and history of previous mental health problems (p<0.01) were most strongly associated with anxiety or depression. Thematic analysis of interviews with women (n=20) identified three themes: ‘past present and future’; ‘expectations and control’; and ‘knowledge and conversations’. Questionnaires were completed by 145 midwives. The three themes identified from the focus groups with midwives were: ‘conversations’; ‘it’s immensely complex’; and ‘there’s another gap in their care’. Conclusion: Prevalence rates of anxiety and depression amongst women in early pregnancy were found to be similar to those reported in the literature. Low self-efficacy and previous poor mental health were significant predictors of anxiety and depression. Continuity and more time at appointments were suggested by midwives and women to improve discussions regarding mental health. Midwives were keen to support women but lacked knowledge and confidence. Consistent reference was made to the need for training regarding the practical aspects of supporting women’s mental health.
Nicola has a series of journal papers lined up from her doctorate, with the one I’ve linked to above (‘Prevalence and predictors of poor mental health among pregnant women in Wales using a cross-sectional survey’) being just the first.