A particular aim of mine in starting this blog was to bring research I have been involved in to a wider audience. So with this in mind, here is a post introducing readers to a series of studies I worked on, with Cardiff colleagues, from the late 1990s to around 2006.
The All Wales Community Mental Health Nursing Stress Study was our first project, led by Professor Philip Burnard. Included in the team were Deborah Edwards, Dave Coyle, Anne Fothergill and myself. Our funding was from the GNC for England and Wales Trust, and we aimed to find out about the causes, moderators and outcomes of stress in community mental health nurses (CMHNs) working in Wales. Our data were generated using a demographic questionnaire and these previously created measures:
Maslach Burnout Inventory
General Health Questionnaire (GHQ-12)
Rosenberg Self-Attitude Questionnaire
Community Psychiatric Nursing Stress Questionnaire (Revised)
Psychnurse Methods of Coping Questionnaire
Our first published paper was this literature review, which Scopus tells me has thus far been cited in 66 subsequent publications. We went on to publish a series of data-based articles from the study, in some of the journals whose names I have added to the word cloud above. The references for these papers are listed here, along with a brief summary of our headline findings.
The team’s next study was a systematic review of stress management in the mental health professions. This was funded by the Wales Office of R&D for Health and Social Care, which was the predecessor body to NISCHR. We found far more papers describing how stressed people are than we found papers suggesting solutions to this problem. Follow this link for a reference list and project summary.
Finally in this series of projects was a study ‘to identify the factors that may influence the effectiveness of clinical supervision and to establish the degree to which clinical supervision might influence levels of reported burnout in community mental health nurses in Wales, UK‘. An expanded team this time included Linda Cooper, John Adams and Tara Jugessur. This study involved the distribution of two questionnaires, again to community mental health nurses in Wales:
In the years since this last project concluded I have had conversations with people on what the next line of inquiry might be. The questions we first asked some 15 years ago seem to me to be as relevant today as they were then. I imagine there remain large numbers of very stressed and burned-out mental health practitioners out there. I also suspect there is still work to do to protect the well-being of staff, and to promote their resilience.
Here’s a quick plug for the Mental Health Nurse Academics UK blog, which the group’s chair Michael Coffey has recently launched and is in the process of actively promoting. Hopefully this is a site which will grow over time, receiving contributions from across the MHNAUK membership. As a taster, here’s what’s currently on the ‘Research’ page:
Yesterday Mental Health Nurse Academics UK met at Liverpool John Moores University, for its third and final meeting of this academic year. Hosts were Lisa Woods and Grahame Smith, and the chair was Michael Coffey. In the first part of the day Grahame and Lisa gave an excellent presentation on their cross-European Innovate Dementia project. Business items included updates on plans made at the previous MHNAUK meeting held in March in Cardiff. Andy Mercer presented findings from his and Karen Wright‘s survey of the methods used by universities to select new students of mental health nursing. Fiona Nolan asked members of the group for their suggested items to be included in her forthcoming research expertise, interests and capacity mapping exercise. This will be useful indeed, and at some point soon we will have a better idea of the full range of mental health nursing research being conducted within the UK’s universities.
Mind is today calling for the government and NHS England to put an end to life-threatening face down restraint of people with mental health problems in healthcare settings. Data secured by Mind under the Freedom of Information Act reveals that at least 3,439 patients in England were restrained in a face down position in 2011-12, despite the increased risk of death from this kind of restraint.
‘Dirty work’ involves doings things which are in some way tainted or shameful, but which might still have to be done. A professional group’s dirty work is not the first thing its members typically like to talk about when asked to describe what they do. When mental health nurses present themselves to others it is the helping relationships they build, the listening they do and the recovery they promote that are more likely to feature. My guess is that experiences of holding, secluding and forcibly medicating people are not things that nurses immediately volunteer.
Because dirty work can sometimes feel degrading and morally suspect it can feel easier not to talk about it at all. The good news in mental health nursing is that there are plenty of people interested in describing, researching and questioning the more coercive and controlling aspects of what we collectively do. Len Bowers and Joy Duxbury are examples. In addition to calling for a ban on face-down restraint, in its news release yesterday Mind pressed for the implementation of national standards and accredited training in this area. Nurses have a big part to play in the debates which are to follow and in developing new practices, and I’ll be watching with interest.
The formal academic year for students of the health professions (and therefore for their teachers, too) tends to be on the long side. Whilst many UK university students will have ended their studies until the autumn there are plenty of nurses, midwives and others with work to do before they can knock off for the summer. In September I’ll be working with pre-registration, second year, students of mental health nursing in a module assessed through the critiquing of published research. Before then I have a short, intensive, module to lead which is part of the taught component within the School’s professional doctorate.
This doctoral level module is all about ‘complexity’ and ‘systems’ and starts next month, and today I’ve been putting the finishing touches to some of the materials I’ll be using. As befits the student group and their thesis-producing aspirations I have opted to draw heavily on colleagues’ and my research experiences as far as is possible. I’m also hoping to foster a spirit of studying and learning together, and want to avoid being didactic.
Elsewhere today, in addition to research project-related work, I have had the opportunity to be part of a panel considering applications for RCN Foundation bursaries. There were some strong candidates, and well done to all who are about to get letters confirming their success. Others will be invited to interview (which I personally am unable to take part in). My commiserations, too, to those dropping out at this stage. I know how it feels to apply for support and not to get it, but there are always other opportunities. As I once heard someone, somewhere, say: if you’re not getting funding bids rejected you’re not applying enough!
A series of train journeys home gives me space to mull over two days spent in London. Yesterday opened with a meeting of the COCAPP Lived Experience Advisory Group (LEAG), expertly chaired by the wonderful Alison Faulkner. Significantly, key parts of COCAPP are changing in response to LEAG recommendations. Our semi-structured interview schedules, for example, directly reflect the LEAG’s input. This is all good, and I am personally learning huge amounts from the opportunity to be involved.
As entirely anticipated Alan gave an informed, engaging and challenging talk, which took in his personal journey into mental health nursing and conveyed key messages from his research. Alan gave us plenty to think about. Might peer support workers be attractive to managers with squeezed budgets? Might they begin to replace members of more established groups, nurses included? Or, as Alan hoped, can peer support workers, nurses and others work side-by-side in harmonious fashion for the benefit of people using services?
Malcolm Rea I do not personally know, though based on the talk on leadership in mental health nursing he gave yesterday this has been my loss. I shall remember his contrasting of ‘drains’ and ‘radiators’ (and try personally to be more of the latter than the former).
Yesterday ended with a convivial social in a London pub, and today was more COCAPP: this time a team meeting followed by a Project Advisory Group (PAG) skillfully chaired by John Larsen from Rethink. Some of our discussion centred on the finer aspects of COCAPP’s design and methods, and for that the study will benefit.
So there we are then: only the shortest summary of some pretty involved discussions, but it will do for now. Home calls.
Just enough time for me to draw attention to some important happenings about to take place in the world of mental health nursing. Tomorrow evening (June 12th) Alan Simpson delivers this year’s Skellern Lecture and Malcolm Rae receives his Journal of Psychiatric and Mental Health Nursing Lifetime Achievement Award. Here are the flyers for these linked events, both taking place at City University London:
Not much time for adding to the blog at the mo’, but enough to note that it was good to have spent this morning with the MHRNC Service User and Carer Partnership Research Development Group. This is an important initiative, and today’s meeting brought together user representatives, charity sector staff, colleagues from Involving People and academics. I’m something of a late arrival to the group, and lots of interesting work has already been done: including a research priority-setting exercise. More to follow in due course, I’m sure.
Here’s what will probably be a final Hay Festival-related post. Last Thursday the Nobel Laureate Professor Sir John Sulston chaired a discussion titled The Next Big Thing. This began with four researchers talking about what they do: Alison Rust, a volcanologist; Zita Martins, an astrobiologist; Nicole Grobert, a nanotechnologist; and Jenny Nelson, a physicist working on materials for solar cells.
All gave fascinating talks, and exemplified the art of conveying complex ideas to the interested but non-specialist listener. And who doesn’t want to hear about supervolcanoes (for the record, they’re bad news, and are definitely best avoided)? Or amino acids from space, the practical applications of graphene or comparing different ways of capturing energy from the sun?
This discussion has since got me thinking about the Next Big Things in nursing and midwifery research (and mental health nursing research in particular). Generally nurses do not do fundamental or basic science, and are not in the business of discovering how bits of the natural world work. So, no volcanoes or extraterrestrial chemicals for us. But practical applications of health-related technologies, and exploring and comparing different ways of doing health work? That’s more up our street, I think, even if graphene and solar power are unlikely to immediately feature.
River Wye, Builth Wells
To the applications-of-technology and exploring-and-comparing questions which might be asked within mental health nursing I would personally add some others related to the examination of health and health care experiences. We know that mental health nurses do ‘people work’ in a big way, spend much of their time coordinating (or ‘articulating’) complex trajectories of care and are often present during service users’ critical junctures. There are applications of skill and technology in this, and how nurses do their work and the effects this has are wide-open areas for study. COCAPP, as I’ve mentioned on this site before, is aiming to distil the components of care planning and care coordination associated with recovery-oriented and personalised mental health services, and is a great example of applied research in this broad field. I’d like to think that its findings will, in some way, be directly useful to practitioners and others in the fullness of time.
Thinking of Graham Thornicroft’s recent editorial on the poor physical health of people using mental health services, referred to on this blog here, if asked to give their research priorities now perhaps some would make a case for researchers and practitioners to combine their efforts to seriously improve this situation. I know there are people working in this area already, but given the magnitude of the problem it seems to deserve some serious new investment. And how about extending research into the mental health nursing contribution to the vital care of older and vulnerable people, including those with dementia? Again, there are people, such as John Keady, doing this already, but possibly not in sufficient numbers. Or research in the area of quality improvement and safety? And what about workforce research, including studies into factors sustaining nurses’ resilience to provide care in conditions of adversity?
However they might be identified and emerge I suspect that any Next Big Thing candidates for nursing research will be the products of sustained collaborations. To return to last Thursday’s four discussants at Hay: all were explicit about interdisciplinarity, and the importance of crossing boundaries to do high quality research aimed at answering ‘big questions’. There are established academic mental health nurses doing this already (I’m thinking of people like Len Bowers, Karina Lovell, Patrick Callaghan and Alan Simpson), but more of us need to make friends with colleagues possessing specific substantive and methodological expertise relevant to our intended studies. Depending on the questions at hand this might mean finding collaborators with disciplinary backgrounds in various of the social and physical sciences and in the humanities, and if necessary with experience in the practical conduct of clinical trials, qualitative investigation and so on. Crucially, and arguably most importantly, it also means forging meaningful collaborations with people with experience of using services, whose priorities are the ones which really matter.
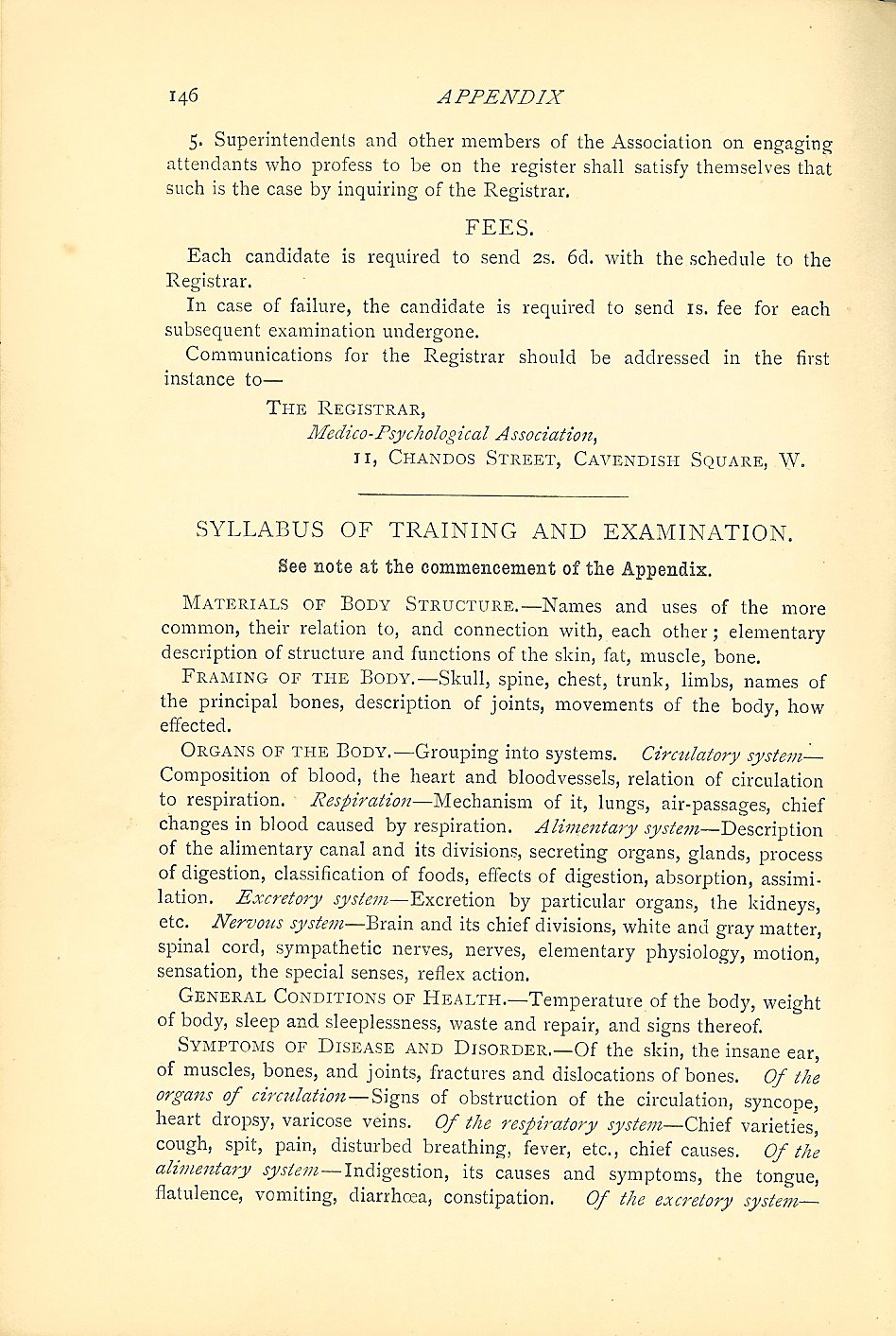
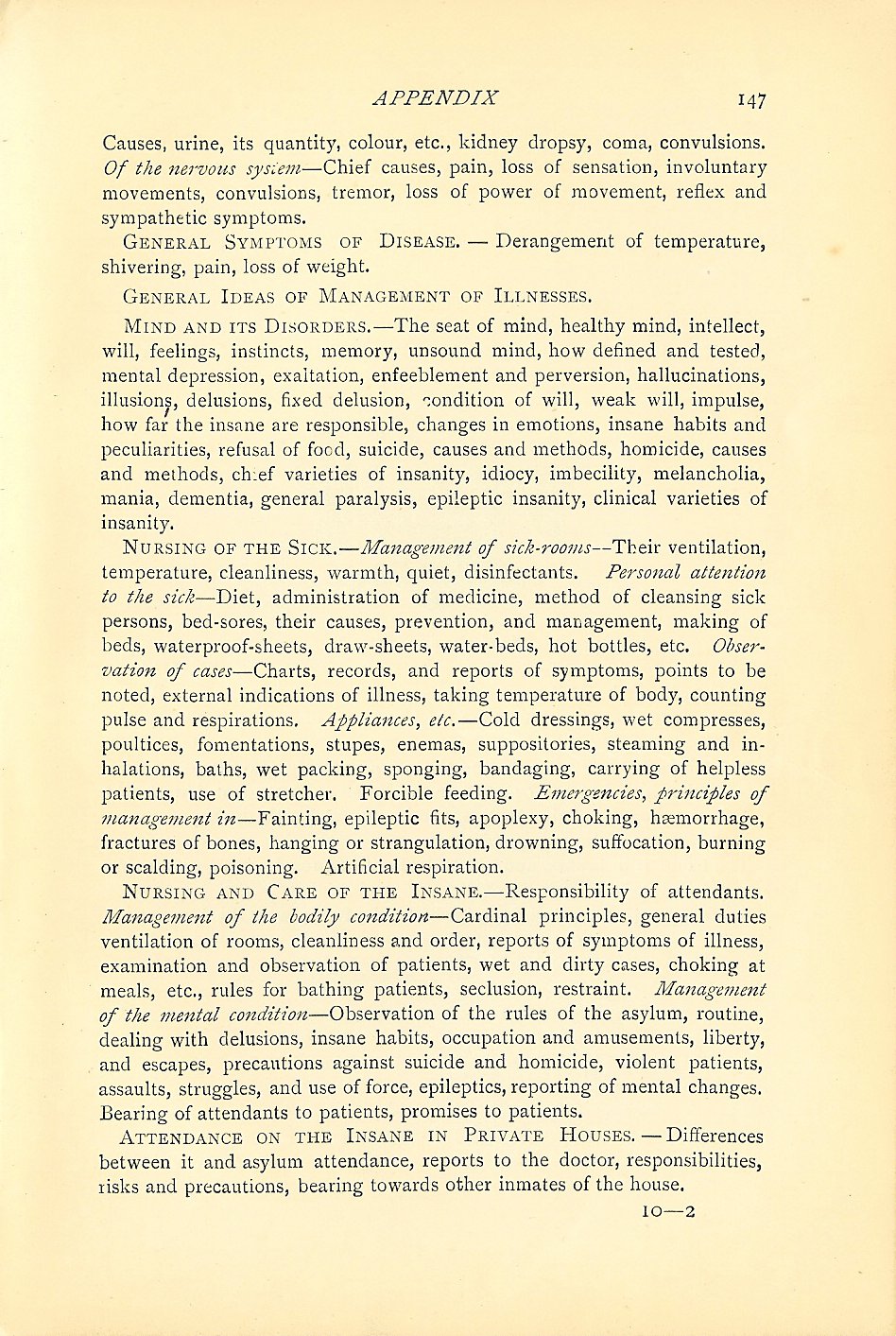
For students up and down the country it is examination season. Whilst students of mental health nursing are busy submitting their dissertations, writing up their reflective essays and achieving their practice-based ‘competencies’ I thought it might be interesting to share the ‘Regulations for the Training and Examination of Candidates for the Certificate of Proficiency in Nursing and Attending on the Insane’. I have scanned these from my copy of the Red Handbook:
In uploading these pages I have just noticed the mention (on page 147, the last-but-one reproduced above) of ‘Attendance of the insane in private houses’. Is it stretching things too far to suggest this as an early reference to community mental health nursing?
I also notice how much these regulations refer to the assessment and maintenance of bodily health (although I have no idea whatsoever what might be meant by ‘the insane ear’, a phrase appearing on page 146). Earlier this week, writing in an editorial for the BMJ Graham Thornicroft described the excess mortality of people with mental health problems as ‘a human rights disgrace’. He’s right, and whilst I’m glad we’re out of the age of the asylum and of ‘attending on the insane’ we might yet learn something from an historic nursing syllabus which placed emphasis on the importance of physical well-being.
 A particular aim of mine in starting this blog was to bring research I have been involved in to a wider audience. So with this in mind, here is a post introducing readers to a series of studies I worked on, with Cardiff colleagues, from the late 1990s to around 2006.
A particular aim of mine in starting this blog was to bring research I have been involved in to a wider audience. So with this in mind, here is a post introducing readers to a series of studies I worked on, with Cardiff colleagues, from the late 1990s to around 2006.
 Yesterday
Yesterday